He seems nice 

And Doc Hudson showed up! #eyesondesign



Porsche has won many races but this aluminum 356 was the first car to win. One of sixteen.



Why would you want a race car with an automatic transmission?
So the driver can operate the aerodynamics with their left foot.
Wait…what?
So the driver can operate the aerodynamics with their left foot.
Wait…what?


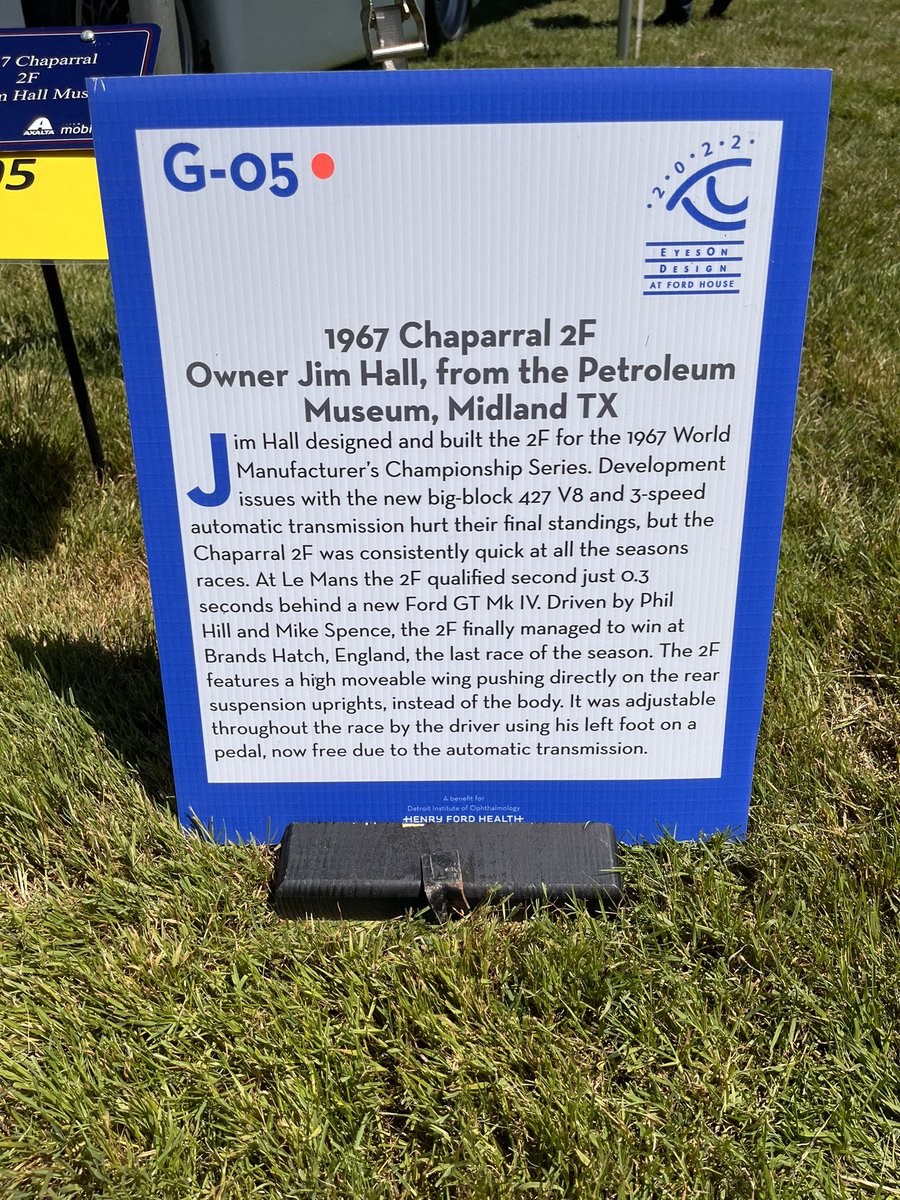
Differential between the legs. Wow.



• • •
Missing some Tweet in this thread? You can try to
force a refresh