Sigh. 🧵
* Viruses don't automatically or inevitably evolve to become milder. Transmissibility and immune escape can be under strong selection but virulence may not be, especially if there are lots of hosts, transmission is easy, and infectiousness precedes symptoms.
* Viruses don't automatically or inevitably evolve to become milder. Transmissibility and immune escape can be under strong selection but virulence may not be, especially if there are lots of hosts, transmission is easy, and infectiousness precedes symptoms.
* Herd immunity isn't going to happen when new immune escaping variants evolve continually. This is true for any source of temporary immunity, but vaccination, infection, or hybrid immunity (vaccination + infection).
* Reinfections are not rare and will probably get more common as vaccine immunity wanes and new variants escape immunity.
* They're all "subvariants of Omicron" in name only. Genetically and antigenically, the various "Omicrons" are quite divergent.
* They're all "subvariants of Omicron" in name only. Genetically and antigenically, the various "Omicrons" are quite divergent.
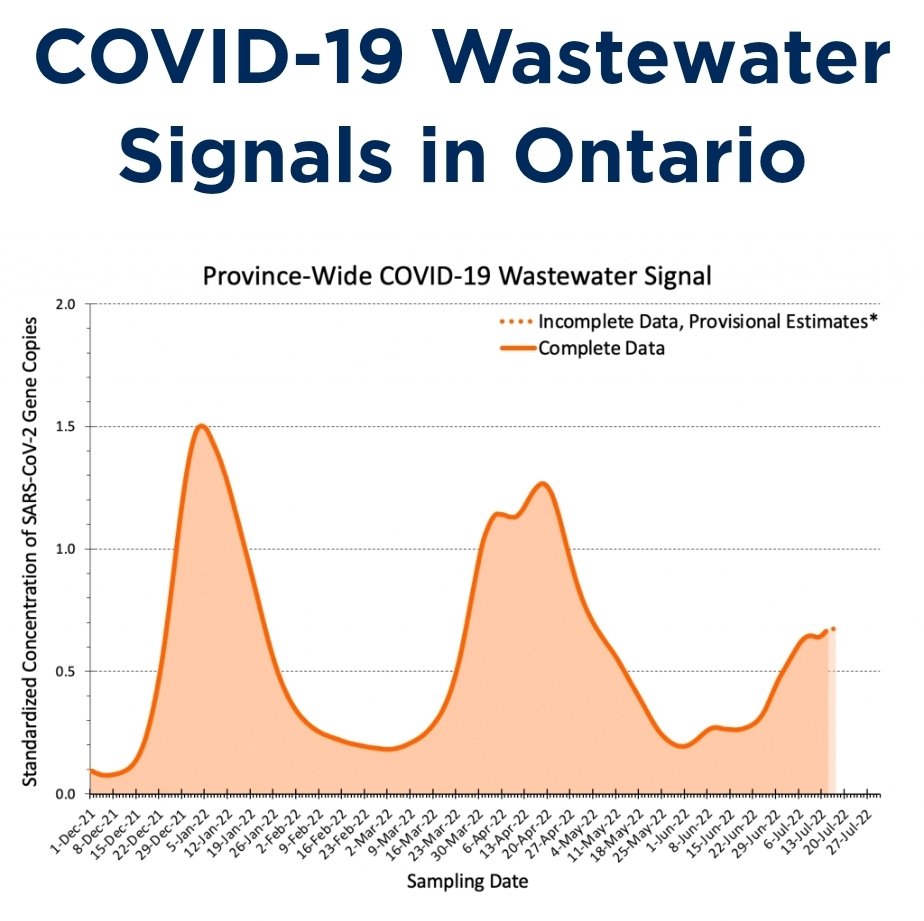
* There's no guarantee that SARS2 will become seasonal on its own. It has become *less* seasonal with recent variants. In many places, we're on the third wave in 7 months.
* The virus is not going to run out of evolutionary space soon. Yes, there is finite variability possible with a small genome, but a lot of room within that for mutations that confer immune escape. The immune landscape keeps changing, so what doesn't work now could work later.
* be it
* No, R0 does not keep going up and up and up with every new variant. Escaping prior immunity can give a relative advantage to a new variant versus the dominant variant in the current host environment but not involve any absolute increase in how transmissible or infective it is.
* The original vaccines still work well to prevent serious illness and disease, even against new variants. But boosters are needed as immunity wanes. Current vaccines were developed for original SARS2 so we need updates, preferably ones that also block transmission (eg nasal).
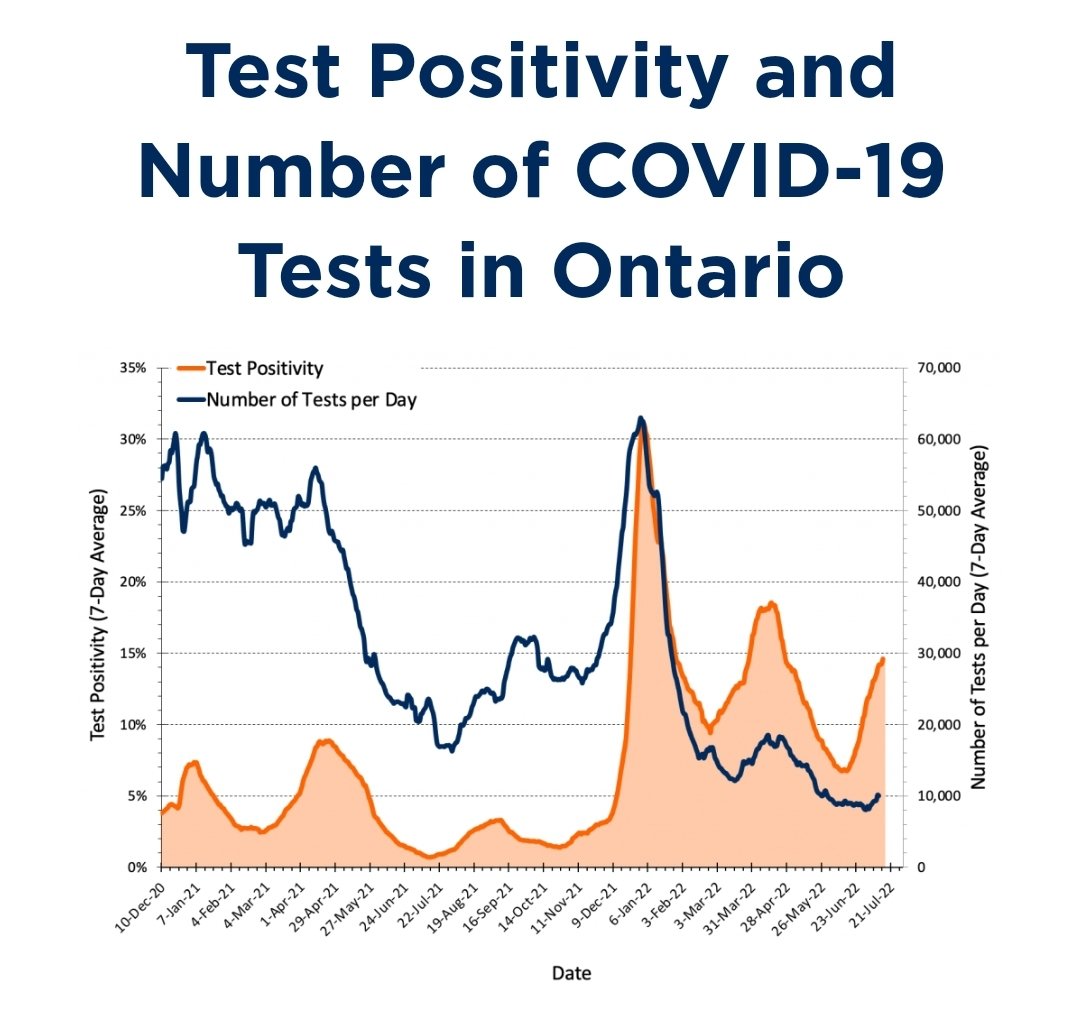
* Cases are not reliable anymore because testing has been reduced so much in most places.
* Deaths are not the only metric of concern. Hospitalizations matter a lot for a number of reasons and can indirectly affect anyone who needs care for any reason.
* Deaths are not the only metric of concern. Hospitalizations matter a lot for a number of reasons and can indirectly affect anyone who needs care for any reason.
* Long COVID is not rare and can affect all kinds of systems.
* It doesn't matter if each reinfection is worse than, the same as, or less severe than prior infections. More infections is worse than fewer infections which is worse than no infections.
* It doesn't matter if each reinfection is worse than, the same as, or less severe than prior infections. More infections is worse than fewer infections which is worse than no infections.
* Good masks worn properly, ventilation, and air filtration work against all current and future variants.
* Washing hands, wiping surfaces, plexiglass barriers, and masks worn under the nose do not stop transmission of airborne viruses.
* Washing hands, wiping surfaces, plexiglass barriers, and masks worn under the nose do not stop transmission of airborne viruses.
Now, if I have got anything wrong about basic immunology, epidemiology, medicine, or engineering mentioned in this thread, I welcome corrections from experts in those fields. Likewise, I will continue to call out evolutionary misconceptions by non-experts.
* serious illness and death
• • •
Missing some Tweet in this thread? You can try to
force a refresh