Impaired Ca2+, TRPM, & LDN in Long Covid & ME/CFS?
Recent reports suggest an overlap in pathology b/t #LongCovid & #ME. Both purportedly involve impaired calcium mobilization.
A few introductory & inchoate thoughts below (better formed thoughts later)🧵
abc.net.au/news/2022-08-1…
Recent reports suggest an overlap in pathology b/t #LongCovid & #ME. Both purportedly involve impaired calcium mobilization.
A few introductory & inchoate thoughts below (better formed thoughts later)🧵
abc.net.au/news/2022-08-1…
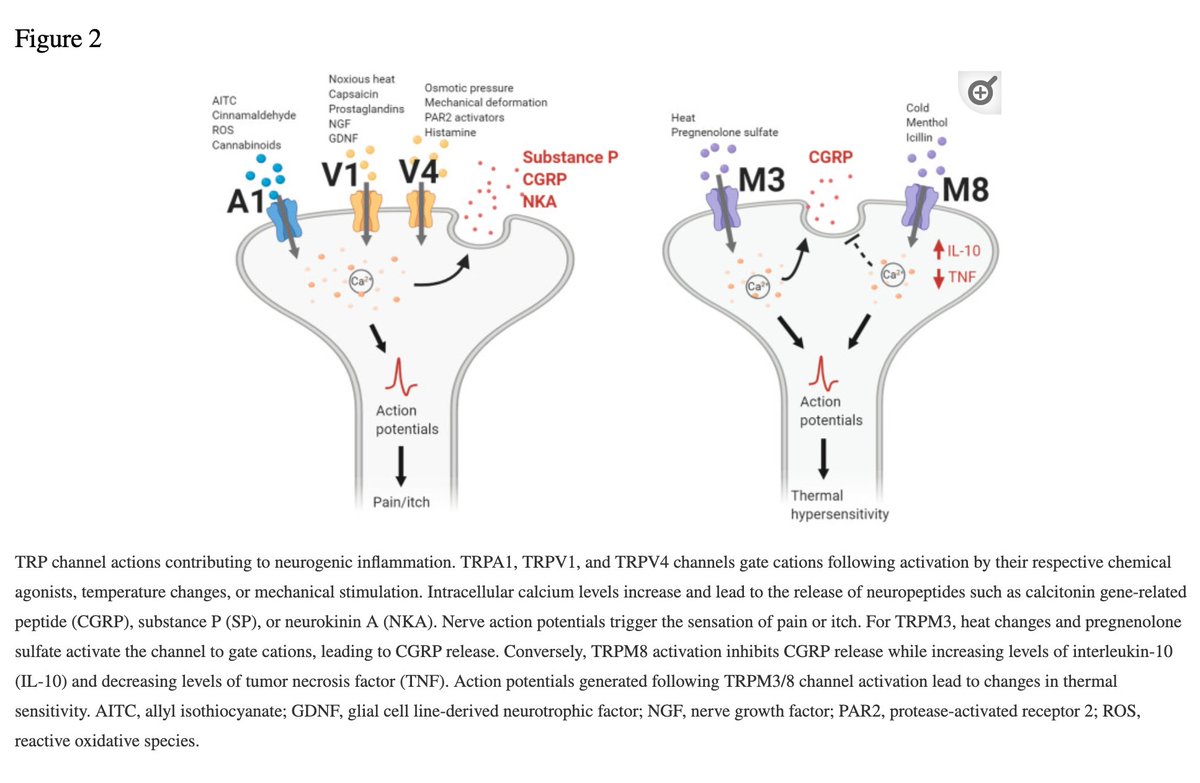
TRPM3 = non-selective ion channel with greatest permeability for CALCIUM
The ion channels form pores on cell surfaces. Upon activation, the cell depolarizes & the pores open, allowing ions to pass through and carry electrical currents.
ncbi.nlm.nih.gov/pmc/articles/P…
The ion channels form pores on cell surfaces. Upon activation, the cell depolarizes & the pores open, allowing ions to pass through and carry electrical currents.
ncbi.nlm.nih.gov/pmc/articles/P…
TRPM3 is expressed in various regions:
kidney >> brain > ovary = testes
It's expressed on peripheral nerves & neurons, “mediating the crosstalk between the nervous system & immune system, particularly in the context of inflammation.”👀
kidney >> brain > ovary = testes
It's expressed on peripheral nerves & neurons, “mediating the crosstalk between the nervous system & immune system, particularly in the context of inflammation.”👀
Multiple studies have shown significant reduction in natural killer (NK) cell cytotoxicity in ME.
A 2016 study found that NK cells showed significantly reduced cytotoxicity in ME/CFS pts compared to healthy controls (17%±2.58% vs 31% ±6.78%).
Why is this relevant?
A 2016 study found that NK cells showed significantly reduced cytotoxicity in ME/CFS pts compared to healthy controls (17%±2.58% vs 31% ±6.78%).
Why is this relevant?
Because these same ME/CFS patients also had mutations (i.e., single nucleotide polymorphisms = SNPs) in 11 TRP ion channels: notably, *five* SNPs associated with TRPM3 and two SNPs with TRPM8, suggesting dysregulation of Ca2+ in TRP ion channel signaling.
pubmed.ncbi.nlm.nih.gov/27099524/
pubmed.ncbi.nlm.nih.gov/27099524/
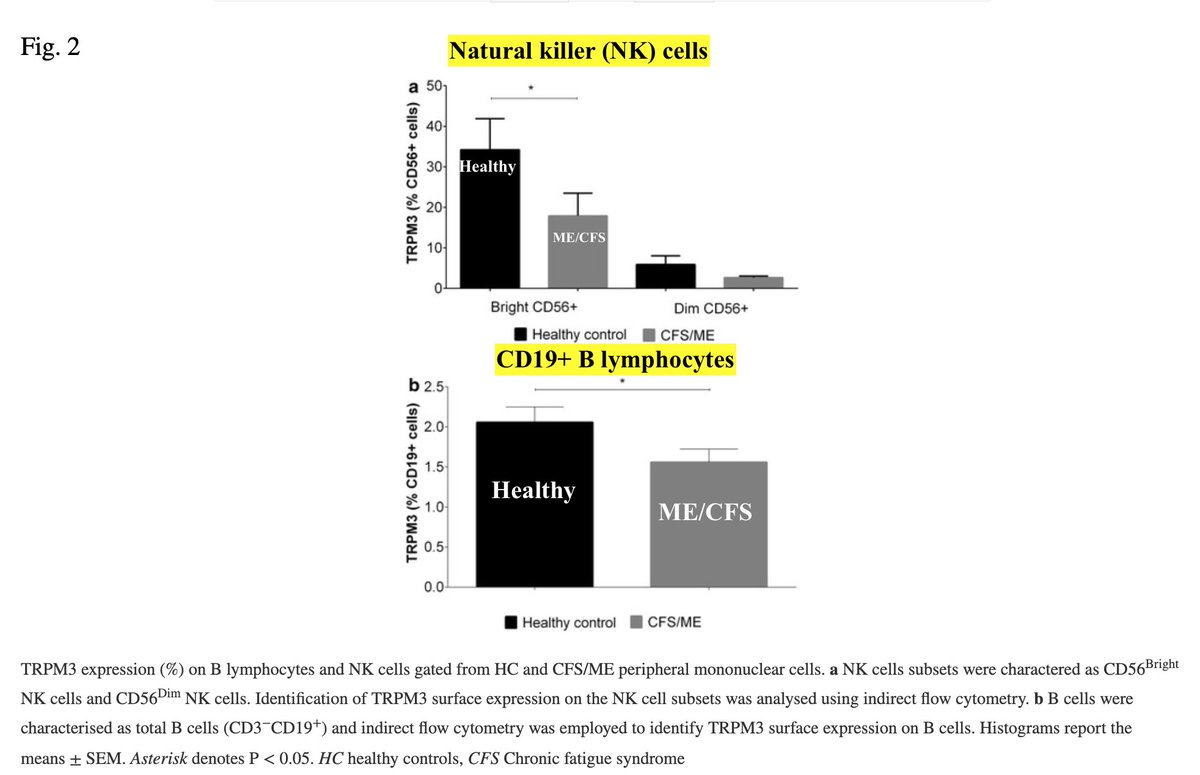
Another 2016 study examined TRPM3 cell surface expression for NK and B cells in 17 ME/CFS pts compared to 19 healthy controls.
In ME/CFS pts, authors found a significant ⬇️ in:
-cytoplasmic Ca2+ in CD19+ B lymphocytes
-TRPM3 surface expression on CD19+ B lymphocytes & NK cells
In ME/CFS pts, authors found a significant ⬇️ in:
-cytoplasmic Ca2+ in CD19+ B lymphocytes
-TRPM3 surface expression on CD19+ B lymphocytes & NK cells
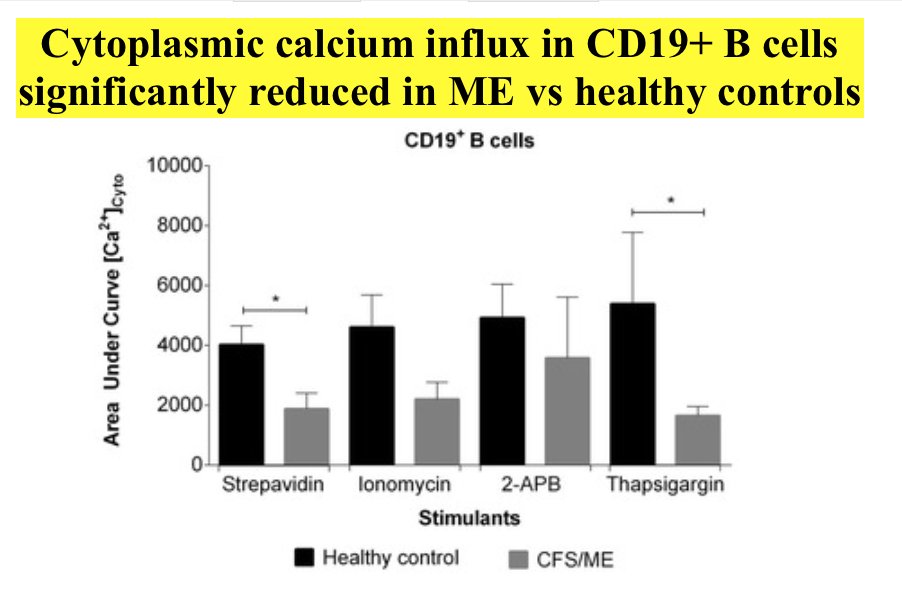
All together, this strongly suggests impaired calcium mobilization in ME/CFS--and perhaps also in Long Covid, considering undeniable similarities and recent reports.
pubmed.ncbi.nlm.nih.gov/27245705/
pubmed.ncbi.nlm.nih.gov/27245705/
A 2019 systematic review of NK cell profile & cytotoxic function in ME/CFS examined 17 observational case control studies.
Authors found that “impaired NK cell cytotoxicity remained the most consistent immunological report across all publications.” ncbi.nlm.nih.gov/pmc/articles/P…
Authors found that “impaired NK cell cytotoxicity remained the most consistent immunological report across all publications.” ncbi.nlm.nih.gov/pmc/articles/P…
Recall that TRPM3 is expressed on peripheral nerves & neurons and mediates crosstalk between the nervous system & immune system. If calcium signaling is dysregulated, could this crosstalk be impaired?
Yes, suggests this 2021 study.
ncbi.nlm.nih.gov/pmc/articles/P…
Yes, suggests this 2021 study.
ncbi.nlm.nih.gov/pmc/articles/P…
The above study identifies two additional key players:
IL-2 and PIP2. (Note that IL-2 ⬆️ NK cell cytotoxicity.)
Authors concluded:
👉🏼TRPM function is tightly regulated by PIP2
👉🏼PIP2-dependent TRPM3 function may be impaired in ME/CFS patients
This leads us a bit astray...
IL-2 and PIP2. (Note that IL-2 ⬆️ NK cell cytotoxicity.)
Authors concluded:
👉🏼TRPM function is tightly regulated by PIP2
👉🏼PIP2-dependent TRPM3 function may be impaired in ME/CFS patients
This leads us a bit astray...
...so I'll come back to this later.
Note possible connection (speculation on my part):
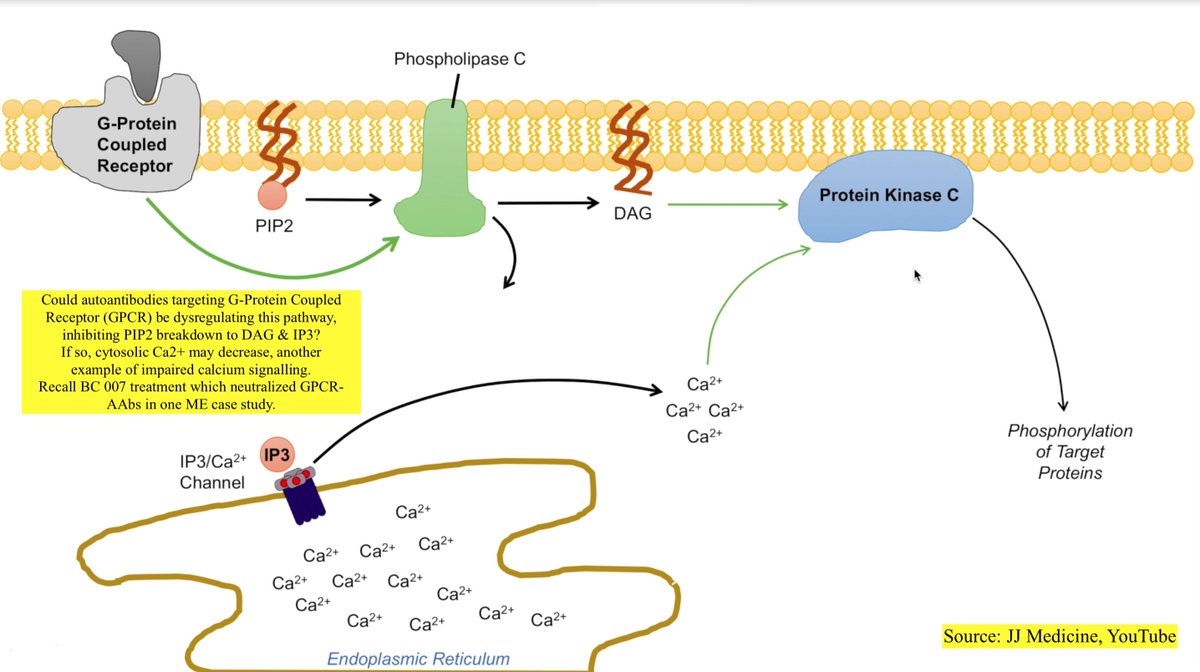
Upon GPCR activation, PLC breaks down PIP2 to IP3 & DAG. IP3 opens Ca2+ channel, releasing Ca2+ into cytosol. If PIP2 dysfunctional, could GPCR auto-Ab be to blame? frontiersin.org/articles/10.33…
Note possible connection (speculation on my part):
Upon GPCR activation, PLC breaks down PIP2 to IP3 & DAG. IP3 opens Ca2+ channel, releasing Ca2+ into cytosol. If PIP2 dysfunctional, could GPCR auto-Ab be to blame? frontiersin.org/articles/10.33…
Back on track:
Low-dose naltrexone (LDN) has shown benefit in Long Covid and ME/CFS, but why?
One major factor relates to TRPM3!
Naltrexone is an opioid antagonist. Opioids agonize (stimulate) µ-opioid receptors (µOR), and µOR agonism inhibits TRPM3.
Low-dose naltrexone (LDN) has shown benefit in Long Covid and ME/CFS, but why?
One major factor relates to TRPM3!
Naltrexone is an opioid antagonist. Opioids agonize (stimulate) µ-opioid receptors (µOR), and µOR agonism inhibits TRPM3.
Importantly, LDN *counteracts* this TRPM3 inhibition.
µOR are also expressed in immune cells where they play immunomodulatory & immunosuppressive roles. Thus LDN may also help NK cell function.
µOR are also expressed in immune cells where they play immunomodulatory & immunosuppressive roles. Thus LDN may also help NK cell function.
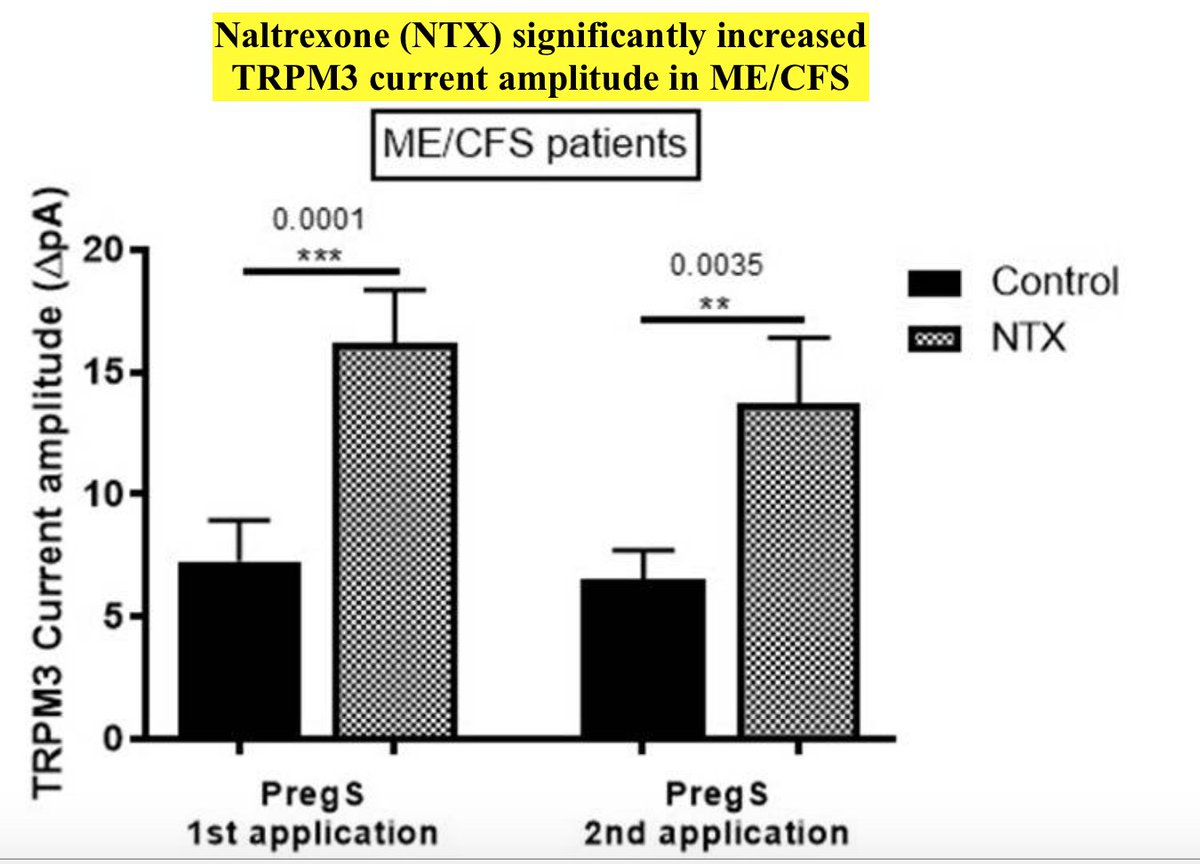
This 2019 study confirmed through electrophysiological investigations that TRPM3 function was impaired in ME/CFS. However, after 24 h incubation w/ naltrexone, TRPM3 channel activity was *restored* in IL-2 stimulated NK cells isolated from ME/CFS patients. ncbi.nlm.nih.gov/pmc/articles/P…
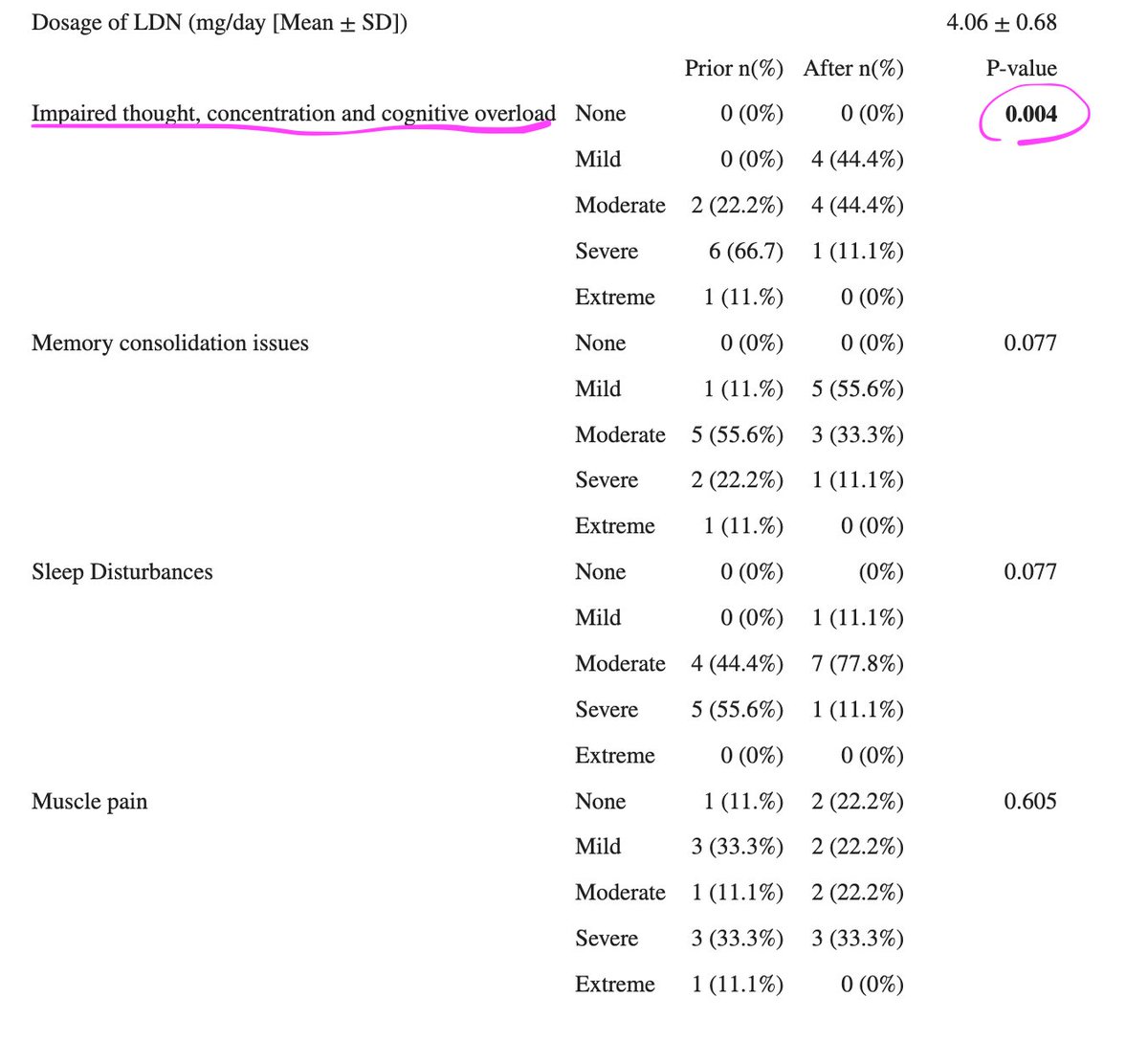
What about symptom improvement? This 2021 study by same authors as above examined the effects of LDN in 9 ME pts. Authors tracked self-reported symptoms before & after LDN treatment. pubmed.ncbi.nlm.nih.gov/31736966/
👉🏼9 ME pts and 9 matched healthy controls (HC)
participated.
👉🏼ME pts had previously started LDN 3-5 mg/day for ≥4
wks.
👉🏼ME/CFS pts reported severity of symptoms prior
to & after LDN trial.
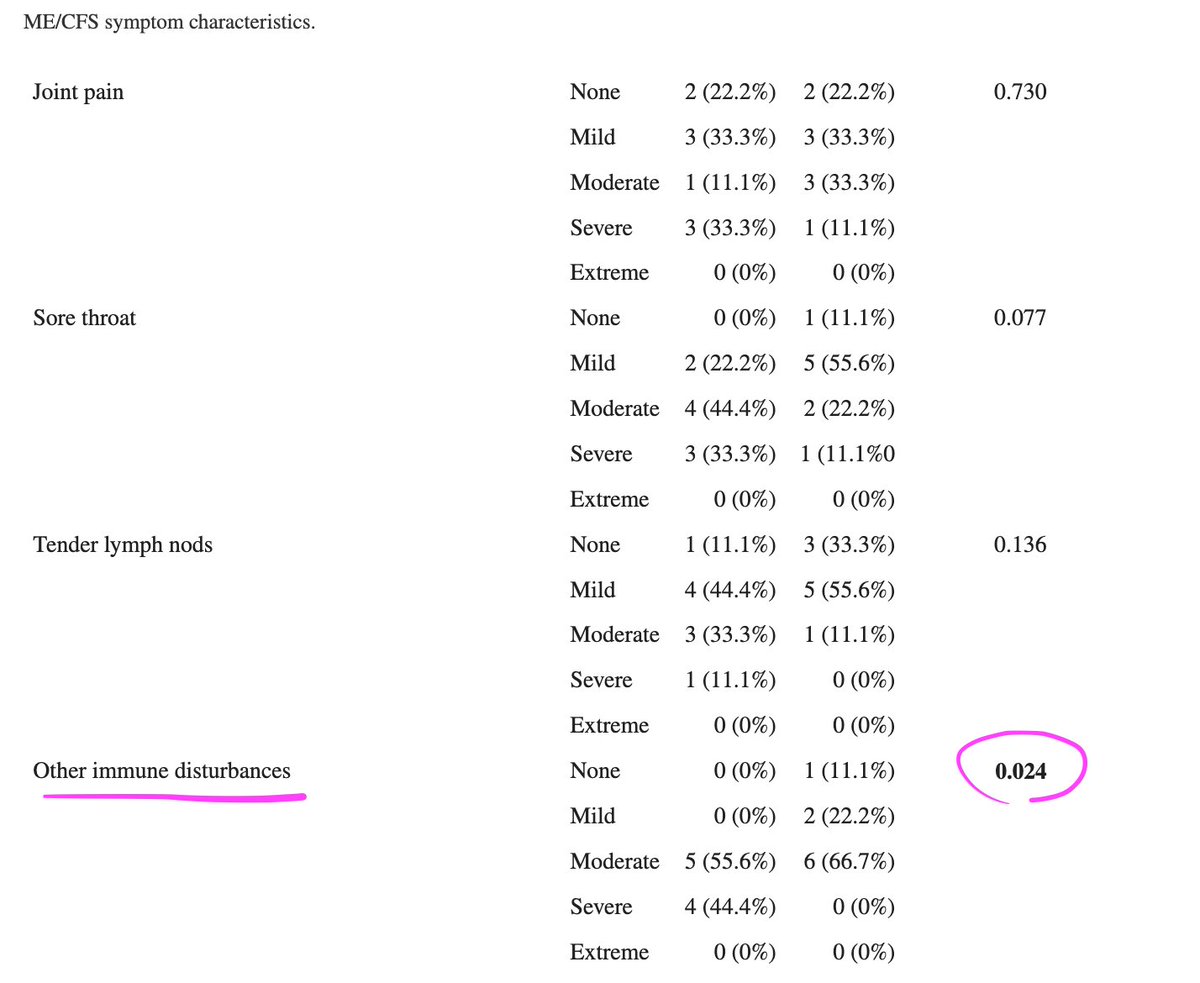
👉🏼Immune disturbances & cognition/concentration sig
improved
participated.
👉🏼ME pts had previously started LDN 3-5 mg/day for ≥4
wks.
👉🏼ME/CFS pts reported severity of symptoms prior
to & after LDN trial.
👉🏼Immune disturbances & cognition/concentration sig
improved
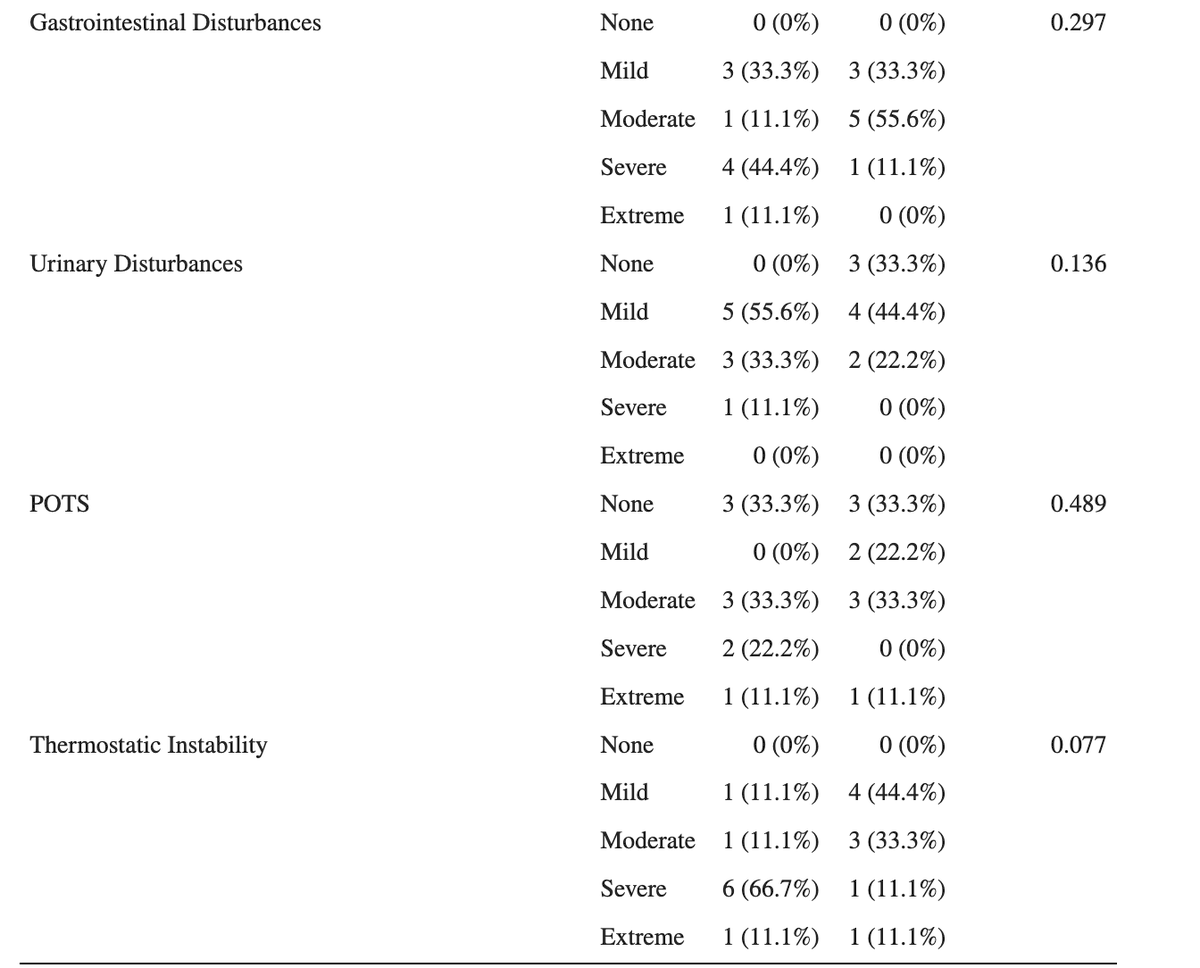
Many other symptoms appeared to improve but the improvements were NOT statistically significant. Note this is based on subjective self-reporting and not objective criteria.
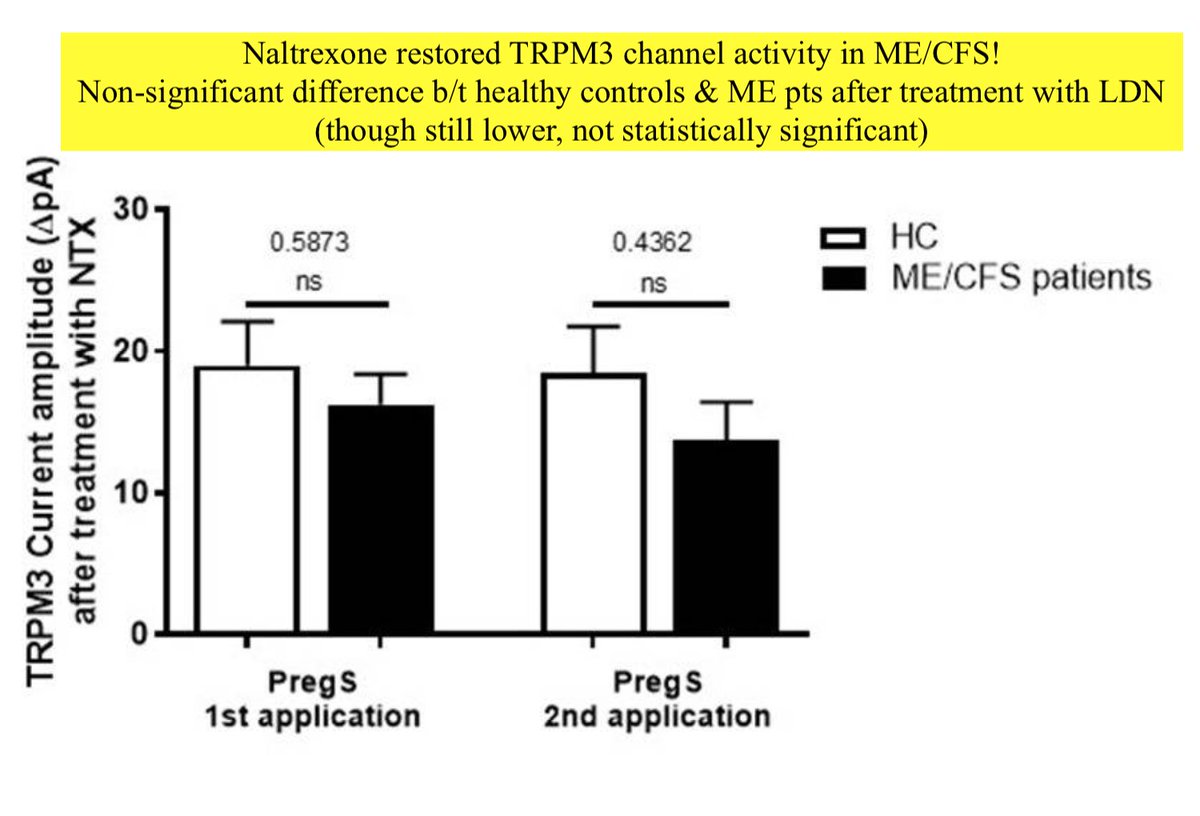
Authors also investigated TRPM3 ion channel activity in isolated NK cells from ME/CFS pts on LDN versus isolated NK cells from healthy controls.
They concluded that "ME/CFS patients taking LDN have restored TRPM3-like ionic currents in NK cells" (won't go into nitty gritty now)
They concluded that "ME/CFS patients taking LDN have restored TRPM3-like ionic currents in NK cells" (won't go into nitty gritty now)
Symptom resolution wasn't too impressive in this study, with only cognition, concentration and unspecified "immune disturbances" improved.
What improvements were in this 2019 retrospective study investigating LDN efficacy in ME?
tandfonline.com/doi/full/10.10…
What improvements were in this 2019 retrospective study investigating LDN efficacy in ME?
tandfonline.com/doi/full/10.10…
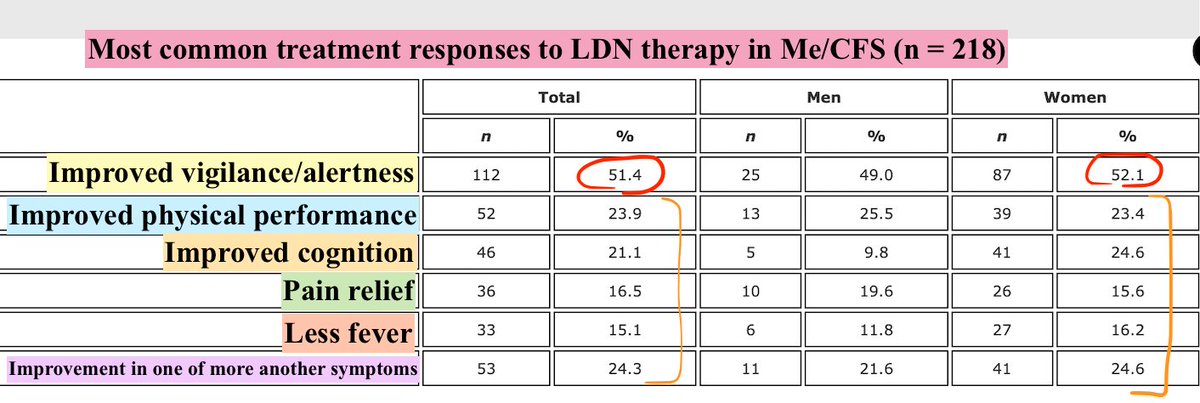
Medical records from 218 ME/CFS patients were analyzed. 74% reported positive treatment response.
However, a breakdown of the responses looks less impressive:
👉🏼“improved vigilance/alertness” only symptom improved in >50%
👉🏼<25% reported improvements in any other symptoms
However, a breakdown of the responses looks less impressive:
👉🏼“improved vigilance/alertness” only symptom improved in >50%
👉🏼<25% reported improvements in any other symptoms
This single center prospective interventional pre post study examined efficacy of LDN in Long Covid patients. Median time from Covid diagnosis until enrollment was 333 days (IQR 171–396). 36 participants (69%) completed a questionnaire after 2+ mon trial.
sciencedirect.com/science/articl…
sciencedirect.com/science/articl…
A significant reduction was seen in low mood, personality change, joint pain, chest tightness & cough (p<0.05).
A trend was seen towards improved fatigue, shortness of breath, brain fog, sleep disturbance, & dysthesia (p<0.10, not statis sig).
Note: there was no control group.
A trend was seen towards improved fatigue, shortness of breath, brain fog, sleep disturbance, & dysthesia (p<0.10, not statis sig).
Note: there was no control group.
TL;DR
1) ⬆️parallels reported b/t ME & LC.
2) One notable similarity involves impaired calcium
3) TRPM3 = calcium-permeable ion channel that shows dysfunction in ME & links to ⬇️NK cytotoxicity
4) LDN may help restore TRPM3 function
5) LDN may weakly improve some ME & LC symptoms
1) ⬆️parallels reported b/t ME & LC.
2) One notable similarity involves impaired calcium
3) TRPM3 = calcium-permeable ion channel that shows dysfunction in ME & links to ⬇️NK cytotoxicity
4) LDN may help restore TRPM3 function
5) LDN may weakly improve some ME & LC symptoms
• • •
Missing some Tweet in this thread? You can try to
force a refresh