
Remarkable day for COVID #rapidtests
A Thread on @US_FDA NEW GUIDANCE!
FDA finally recognized Sensitivity of test *REGIMEN* is as/more important than single test
Sort of recognized virus load goes up & impacts Rapid Tests!
Sounds familiar! (ca 2020)
nejm.org/doi/full/10.10…
1/
A Thread on @US_FDA NEW GUIDANCE!
FDA finally recognized Sensitivity of test *REGIMEN* is as/more important than single test
Sort of recognized virus load goes up & impacts Rapid Tests!
Sounds familiar! (ca 2020)
nejm.org/doi/full/10.10…
1/
OK, So... what did FDA actually say today?
They say if you do not have symptoms
and therefore don't really know where in your infection you are... if at all
and worry you were exposed
And you rapid test Neg... well, test again 2 days later and if Neg.. 2 days later still
2/
They say if you do not have symptoms
and therefore don't really know where in your infection you are... if at all
and worry you were exposed
And you rapid test Neg... well, test again 2 days later and if Neg.. 2 days later still
2/
For anyone following me or the "rapid test discussion" for past 2.5 years... you'll say:
Uhh... well yeah, of course!
Yes this has been obvious since Jan '20
But FDA previously refused to consider "sensitivity of a test regimen" - but only sens of a single test
3/
Uhh... well yeah, of course!
Yes this has been obvious since Jan '20
But FDA previously refused to consider "sensitivity of a test regimen" - but only sens of a single test
3/
This is IMPORTANT
The WHOLE POINT of rapid tests is that, unlike PCR, they can EASILY be used FREQUENTLY after exposure
Since PCR is still Neg for 1-4 days after Exposure
A single PCR is VERY likely to MISS an infection if swabbed too early
And no one "frequently PCRs"
4/
The WHOLE POINT of rapid tests is that, unlike PCR, they can EASILY be used FREQUENTLY after exposure
Since PCR is still Neg for 1-4 days after Exposure
A single PCR is VERY likely to MISS an infection if swabbed too early
And no one "frequently PCRs"
4/
After exposure, virus needs time to grow
PCR stays Neg 1-4 days after Exposure
&
Rapid test for 1-5 days after Exposure
So...Rapid Sounds worse – extra day of being Neg
BUT
Bc can EASILY rapid test multiple times -->
youre MUCH more likely to find infection w rapid tests
5/
PCR stays Neg 1-4 days after Exposure
&
Rapid test for 1-5 days after Exposure
So...Rapid Sounds worse – extra day of being Neg
BUT
Bc can EASILY rapid test multiple times -->
youre MUCH more likely to find infection w rapid tests
5/
We have written about this many times
See @NEJM paper above & this paper from 2020 (now in @ScienceTM) demonstrating w 'mathematical certainty' that for COVID screening,
Test FREQUENCY is much more important than single test sensitivity
science.org/doi/10.1126/sc…
6/
See @NEJM paper above & this paper from 2020 (now in @ScienceTM) demonstrating w 'mathematical certainty' that for COVID screening,
Test FREQUENCY is much more important than single test sensitivity
science.org/doi/10.1126/sc…
6/
Now, FDA's stance has *sort of* changed!
Recently, FDA DID evaluate sensitivity of "multiple tests"
b/c they're FINALLY recognizing that sensitivity of a test has everything to do with virus load, not just "PCR+ status"
7/
Recently, FDA DID evaluate sensitivity of "multiple tests"
b/c they're FINALLY recognizing that sensitivity of a test has everything to do with virus load, not just "PCR+ status"
7/
If youre JUST exposed - No test is Pos
If you JUST turned PCR(+) – rapid can still be Neg for ~1 more day
So, had you just rapid tested 1 day later (b4 you'd normally even get PCR result back)
Rapid would've been (+)
See this chart I made in 2020 (click to see all)
8/
If you JUST turned PCR(+) – rapid can still be Neg for ~1 more day
So, had you just rapid tested 1 day later (b4 you'd normally even get PCR result back)
Rapid would've been (+)
See this chart I made in 2020 (click to see all)
8/

If we compare example chart (drawn in 2020; bottom) w data FDA is finally "recognizing" (top)
You'll see the new data reflects almost exactly what we've known and shown for 2+ years
Sensitivity of the rapid test is ENTIRELY dependent on virus load!
Exactly as expected!
9/
You'll see the new data reflects almost exactly what we've known and shown for 2+ years
Sensitivity of the rapid test is ENTIRELY dependent on virus load!
Exactly as expected!
9/

FDA found
On 1st day of PCR Positive
60% also Pos on Rapid Ag test
but when tested 2 days later
93% were Pos on rapid test!
So, in just 2 days, Sens of rapid Ag test went
from 60% --> 93%
Sensitivity DEPENDS ON VIRUS LOAD!!
(Shouldn't have taken 2+ yrs)
there's more!
10/
On 1st day of PCR Positive
60% also Pos on Rapid Ag test
but when tested 2 days later
93% were Pos on rapid test!
So, in just 2 days, Sens of rapid Ag test went
from 60% --> 93%
Sensitivity DEPENDS ON VIRUS LOAD!!
(Shouldn't have taken 2+ yrs)
there's more!
10/

Further
When COMBINED Rapids from days 0, 2 (& 4)
Sensitivity went
60% --> 98% (& 100%)!!
FINALLY FDA is recognizing this & says:
If you test Pos... done -> you knew in 10 mins instead of days waiting for PCR
But
If Neg & were exposed, Test again in 48 hrs
11/
When COMBINED Rapids from days 0, 2 (& 4)
Sensitivity went
60% --> 98% (& 100%)!!
FINALLY FDA is recognizing this & says:
If you test Pos... done -> you knew in 10 mins instead of days waiting for PCR
But
If Neg & were exposed, Test again in 48 hrs
11/
Essentially
FDA is FINALLY *sort of* formally recognizing that sensitivity is ENTIRELY related to virus load
That rapid tests perform EXTREMELY WELL when it matters most – when virus load is high
Even if they don't perform v well on day 0 when virus load is extremely low
12/
FDA is FINALLY *sort of* formally recognizing that sensitivity is ENTIRELY related to virus load
That rapid tests perform EXTREMELY WELL when it matters most – when virus load is high
Even if they don't perform v well on day 0 when virus load is extremely low
12/
Interestingly, that was for ppl WITH Symptoms
For those w/out Symptoms, they say something different...
They suggest:
IF you were exposed & are Neg on a rapid test ->
Test 48hrs later and if still Neg ->
Test once more 48 hours after that
Why?
13/
For those w/out Symptoms, they say something different...
They suggest:
IF you were exposed & are Neg on a rapid test ->
Test 48hrs later and if still Neg ->
Test once more 48 hours after that
Why?
13/
Well, not surprisingly, they found that some ppl who tested Pos on PCR but had NO symptoms didn't turn Rapid test Pos till 4 days later...
And many NEVER turned Pos
This is FULLY expected!
PCR is SO sensitive it detects virus in ppl who don't ever become infectious
14/
And many NEVER turned Pos
This is FULLY expected!
PCR is SO sensitive it detects virus in ppl who don't ever become infectious
14/
We know this b/c among the 97 "No symptom" PCR Pos ppl, a full 21% only had a SINGLE PCR positive test and were PCR neg 2 days later
Just a blip of PCR Pos -> then cleared
Those ppl were NEVER infectious but b/c PCR, all still had to isolate (a public health FAILURE IMO)
15/
Just a blip of PCR Pos -> then cleared
Those ppl were NEVER infectious but b/c PCR, all still had to isolate (a public health FAILURE IMO)
15/
Given that 20/97 (21%) of those with NO symptoms had only a single blip of PCR
the other 77/97 (79%) likely were along a wide spectrum of virus loads
It's very likely many just had 2 or 3 PCR Pos tests and then never again... those ppl too likely never were infectious...
16/
the other 77/97 (79%) likely were along a wide spectrum of virus loads
It's very likely many just had 2 or 3 PCR Pos tests and then never again... those ppl too likely never were infectious...
16/
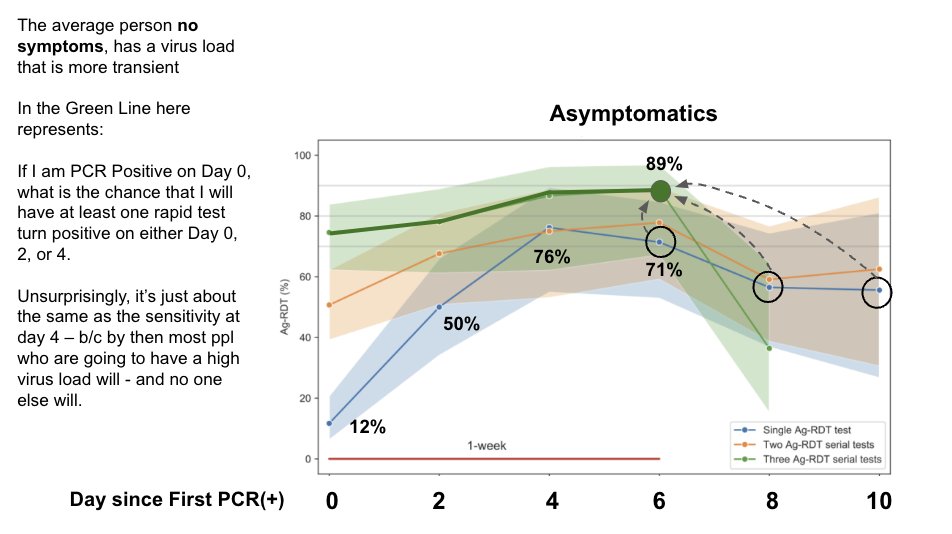
And the study showed exactly this -> that virus load was lower and more transient in Asymptomatics
Reflected in Lower measured sensitivity of rapid tests vs. PCR -> NOT b/c the test didn't work well in Asymptomatics
But Simply bc virus Load was LOWER in this group
17/
Reflected in Lower measured sensitivity of rapid tests vs. PCR -> NOT b/c the test didn't work well in Asymptomatics
But Simply bc virus Load was LOWER in this group
17/

The study FDA evaluated also looked at "cumulative sensitivity" ->
Probability that if PCR Pos on Day 0 (for instance) that a rapid Ag test turn will be Pos on day 0 OR day 2 OR day 4
The cumulative Sens highlights that Asymptomatics have more transient high virus load
18/
Probability that if PCR Pos on Day 0 (for instance) that a rapid Ag test turn will be Pos on day 0 OR day 2 OR day 4
The cumulative Sens highlights that Asymptomatics have more transient high virus load
18/

Here is an explanation of that graph... I highlight how the "cumulative sensitivity" is being calculated. It's a little weird, so I tried to draw it out
This slide explains how the "cumulative sensitivity" is calculated for Day 0 since first turning PCR positive
19/
This slide explains how the "cumulative sensitivity" is calculated for Day 0 since first turning PCR positive
19/

Importantly!!
If No Symptoms and you rapid test on days 6, 8, and 10, your cumulative sensitivity = 89%
vs 71% for day 6 alone
Which means 18% of may only be getting high virus loads that turn Rapid Test Pos after 8 or 10 days!
A HUGE delay - problematic for CDC guidance
20/
If No Symptoms and you rapid test on days 6, 8, and 10, your cumulative sensitivity = 89%
vs 71% for day 6 alone
Which means 18% of may only be getting high virus loads that turn Rapid Test Pos after 8 or 10 days!
A HUGE delay - problematic for CDC guidance
20/
So, Its these results that led FDA to say that to screen...
• If exposed and have Symptoms and Test Neg
-> test 48 hrs later
-> cumulative sensitivity = 98%!
• If No symptoms
–> test 48h and
–> again 48h more
(cumul Sens = 87%)
21/
fda.gov/medical-device…
• If exposed and have Symptoms and Test Neg
-> test 48 hrs later
-> cumulative sensitivity = 98%!
• If No symptoms
–> test 48h and
–> again 48h more
(cumul Sens = 87%)
21/
fda.gov/medical-device…

While I'm glad FDA is FINALLY recognizing that it's best to consider sensitivity of a testing Regimen over time (bc VIRUS LOAD CHANGES w time)
(though they didn't actually admit that is what they are considering)
The guidance and thought process comes unfortunately late
22/
(though they didn't actually admit that is what they are considering)
The guidance and thought process comes unfortunately late
22/
On the Same day the FDA is saying "If asymptomatic, test yourself 3 times with 48 hours apart for each"
The @CDCgov extraordinarily came out w guidance that more or less says "Don't worry if you're Pos - feel free to go infect others if you wish"
(paraphrased of course)
23/
The @CDCgov extraordinarily came out w guidance that more or less says "Don't worry if you're Pos - feel free to go infect others if you wish"
(paraphrased of course)
23/
The dichotomy between the 2:
@CDCgov saying to move on & pretend COVID is behind us (w 1000's of deaths / week still)
&
FDA, just now beginning to catch up to the science we showed them 2+ years AGO
is jarring
Leaves me w little hope for US gov to lead public health
24/
@CDCgov saying to move on & pretend COVID is behind us (w 1000's of deaths / week still)
&
FDA, just now beginning to catch up to the science we showed them 2+ years AGO
is jarring
Leaves me w little hope for US gov to lead public health
24/
The data that FDA largely considered is from this paper by Soni et al.
medrxiv.org/content/10.110…
And FDA new guidance is
fda.gov/medical-device…
I honestly don't have the energy to talk about the absolute shit show that is CDC's new guidance...
25/
medrxiv.org/content/10.110…
And FDA new guidance is
fda.gov/medical-device…
I honestly don't have the energy to talk about the absolute shit show that is CDC's new guidance...
25/
• • •
Missing some Tweet in this thread? You can try to
force a refresh



