I think this paper by the Nielsen group on the use of CT scans to neuroprognosticate after cardiac arrest may be a game-changer.
But it will take a few tweets to explain why... 🧵
pubmed.ncbi.nlm.nih.gov/35931271/
But it will take a few tweets to explain why... 🧵
pubmed.ncbi.nlm.nih.gov/35931271/

prognostication after cardiac arrest involves a structured series of tests performed over time.
this may vary a bit between patients and institutions.
most often, decisions center around the trifecta:
🔺serial clinical examination
🔺continuous EEG
🔺MRI
this may vary a bit between patients and institutions.
most often, decisions center around the trifecta:
🔺serial clinical examination
🔺continuous EEG
🔺MRI

MRI is the weak link:
🖇️ least robust evidence
🖇️ interpretation is subjective
🖇️ logistically challenging (eg pacemaker)
MRI can help if there is *no* anoxia, or if there is an unexpected *alternative* dx.
MRI isn't great at sorting out bad anoxia from moderate anoxia.
🖇️ least robust evidence
🖇️ interpretation is subjective
🖇️ logistically challenging (eg pacemaker)
MRI can help if there is *no* anoxia, or if there is an unexpected *alternative* dx.
MRI isn't great at sorting out bad anoxia from moderate anoxia.
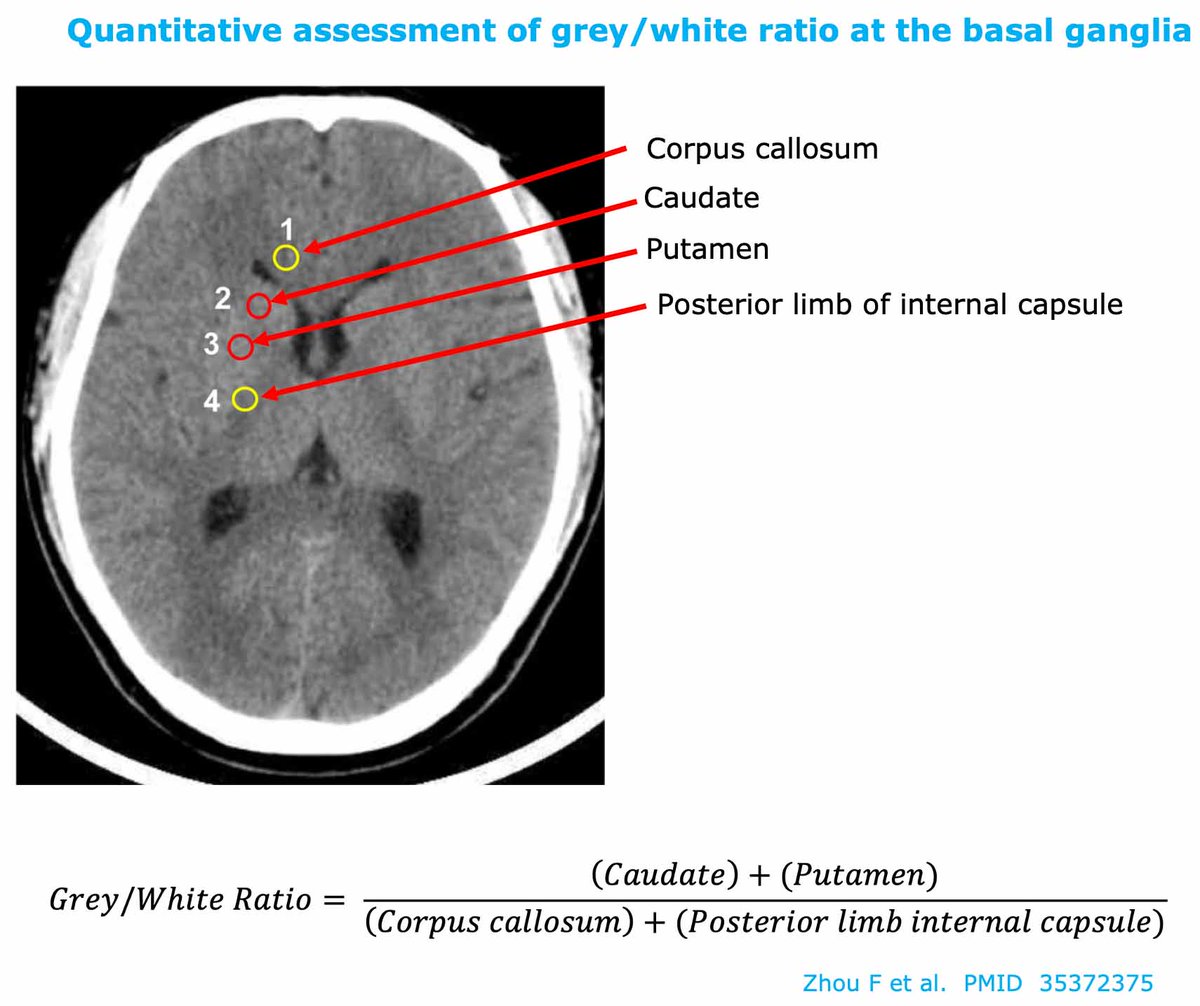
CT has advantages over MRI:
💪 measurement of Houndsfield units allows it to be objective
💪 expanding evidentiary base
💪 high specificity for poor outcome
💪 can be applied to all pts
the problem with CT has been that it's done immediately post-arrest, before edema develops
💪 measurement of Houndsfield units allows it to be objective
💪 expanding evidentiary base
💪 high specificity for poor outcome
💪 can be applied to all pts
the problem with CT has been that it's done immediately post-arrest, before edema develops
the immediate post-arrest CT has poor sensitivity.
but *delaying* the CT >24 hours improves sensitivity, as found in this study from 2018:
but *delaying* the CT >24 hours improves sensitivity, as found in this study from 2018:
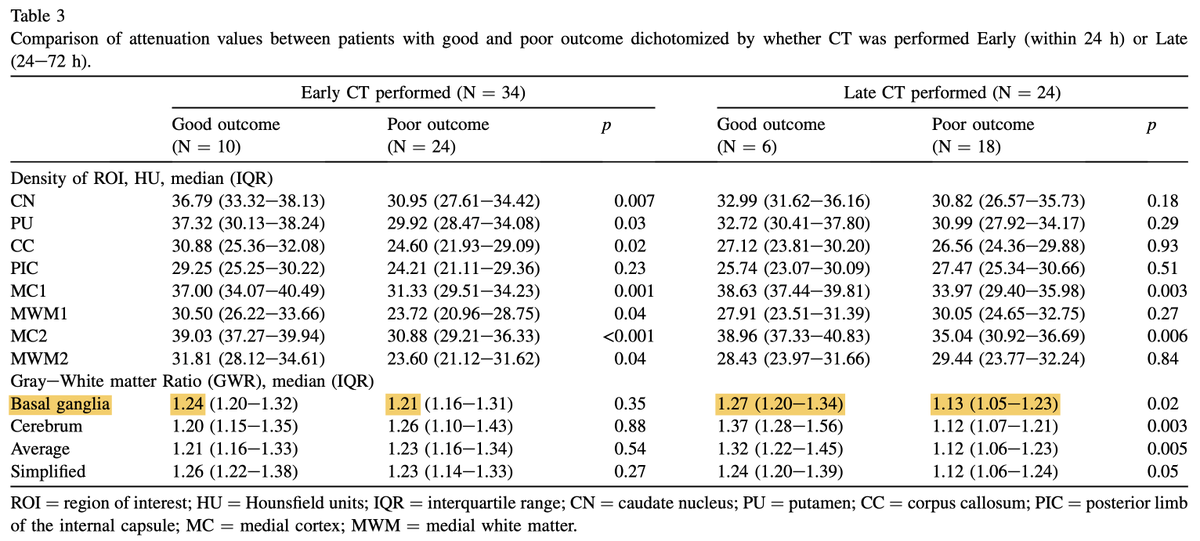
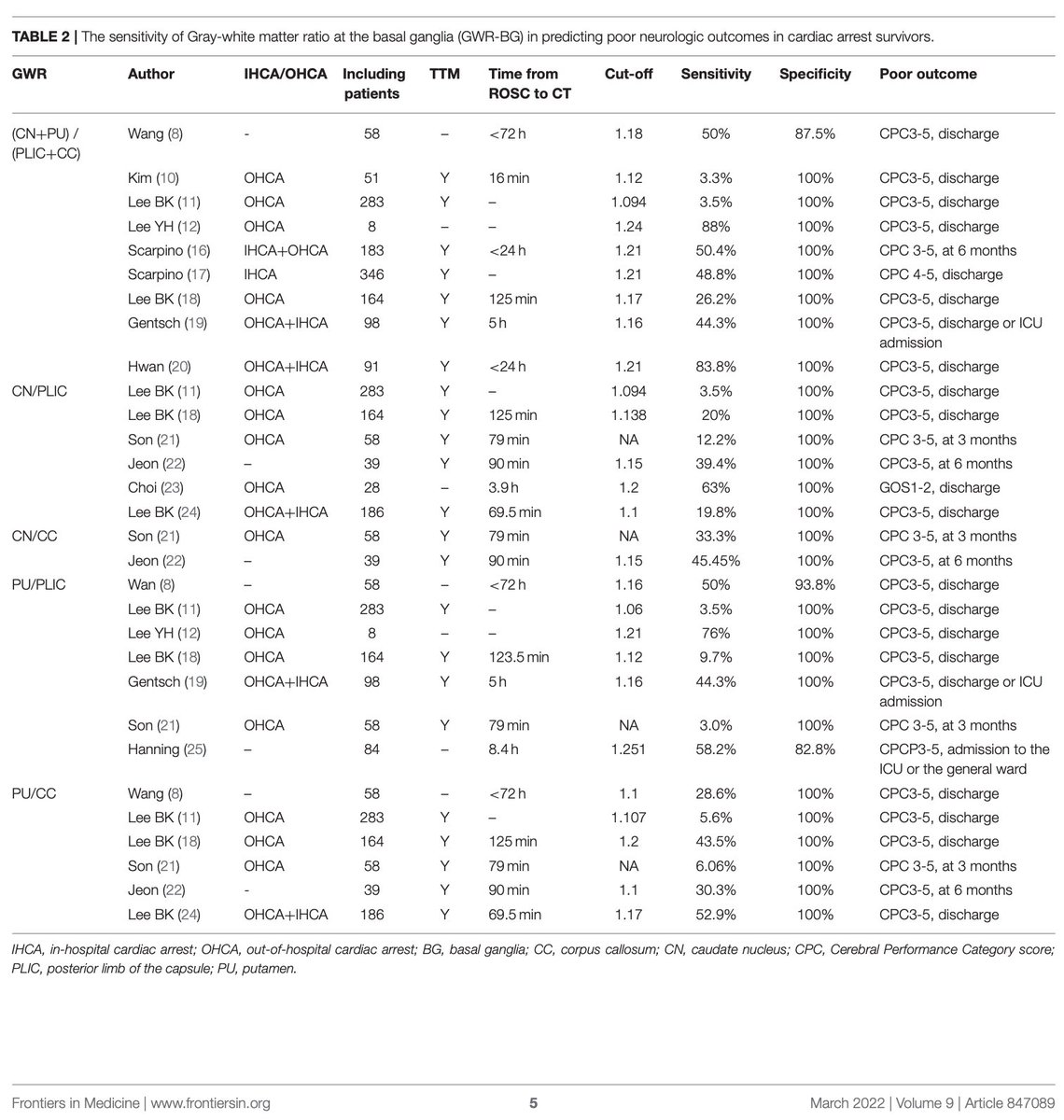
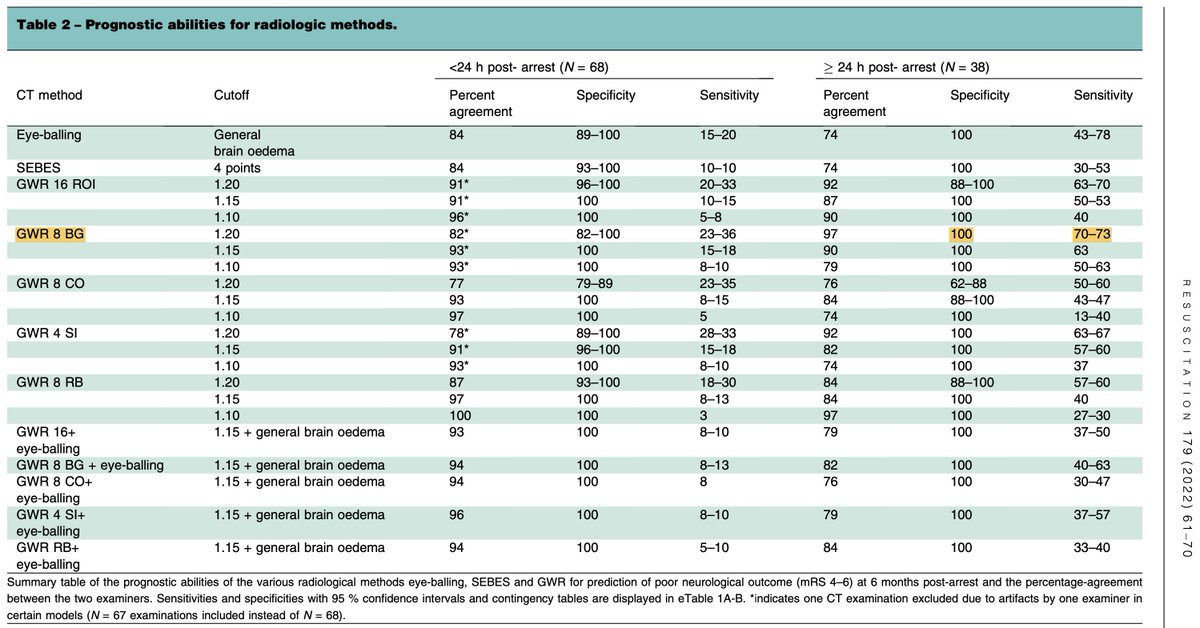
the new study by Nielsen's group extends these findings, by showing that delayed CT scan >24 hr
🐈 ⬆️ sensitivity for severe anoxic injury (~70%)
🐈 retains high specificity for prognosticating a poor outcome
so CT seems to perform very well when evaluated at the right timepoint
🐈 ⬆️ sensitivity for severe anoxic injury (~70%)
🐈 retains high specificity for prognosticating a poor outcome
so CT seems to perform very well when evaluated at the right timepoint
overall, CT scan may be poised to *replace* MRI for post-arrest neuroprognostication in many patients.
of course, each patient must be approached individually
if data isn't lining up (e.g., inconsistencies between exam / EEG / imaging) - wait & get more data!
of course, each patient must be approached individually
if data isn't lining up (e.g., inconsistencies between exam / EEG / imaging) - wait & get more data!
what do folks think about CT-vs-MRI?
the evidence base for CT isn't gigantic, but I think it's better than the data for MRI.
MRI requires subjective interpretation which introduces a source of bias 😤
more on quantitative CT for prognostication IBNCC: emcrit.org/ibcc/np/#CT_sc…
the evidence base for CT isn't gigantic, but I think it's better than the data for MRI.
MRI requires subjective interpretation which introduces a source of bias 😤
more on quantitative CT for prognostication IBNCC: emcrit.org/ibcc/np/#CT_sc…
• • •
Missing some Tweet in this thread? You can try to
force a refresh