ACIP slides: it is a BAD decision to add this to the SCHEDULE 👇
This vaccine has (a) no convincing evidence it helps the 86% of kids who already had covid & (b) no evidence it will help kids in 2027 against whatever new strain comes
CDC data shows parents don't want it🧵
This vaccine has (a) no convincing evidence it helps the 86% of kids who already had covid & (b) no evidence it will help kids in 2027 against whatever new strain comes
CDC data shows parents don't want it🧵

93.1% of parents don't want to vaccinate their young kids
That is for good reason; there is no RCT data this vaccine lowers severe disease in this age group, and even the observational studies I am aware of (flawed) look at 5-11
No study pertains to kids where 86% had covid
That is for good reason; there is no RCT data this vaccine lowers severe disease in this age group, and even the observational studies I am aware of (flawed) look at 5-11
No study pertains to kids where 86% had covid

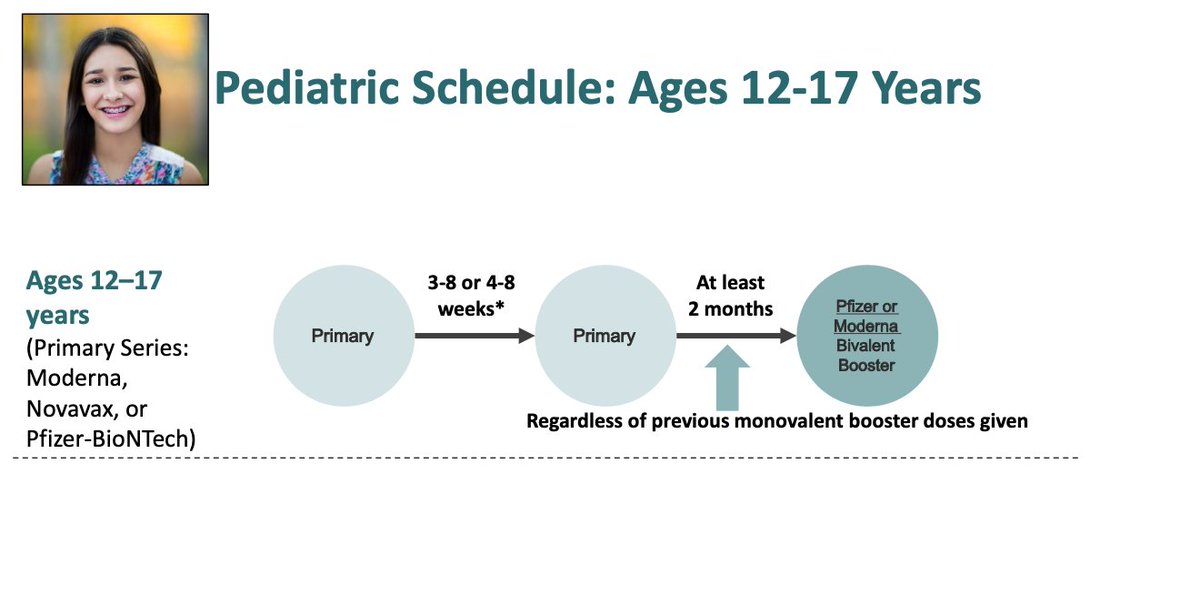
CDC slides also full of errors and bad decisions
They are stacking 2 booster doses in adolescents-- this should raise concern of unnecessary myocarditis that might be averted with omission or spacing the last dose
They are stacking 2 booster doses in adolescents-- this should raise concern of unnecessary myocarditis that might be averted with omission or spacing the last dose
They assert this as fact, but surely at some point the calculus tips
a 20 year old man who got 3 doses and just had OMICRON- benefits from a bivalent booster targetting an earlier strain?
No evidence supports this, and it is nonsensical
What about dose #20?
a 20 year old man who got 3 doses and just had OMICRON- benefits from a bivalent booster targetting an earlier strain?
No evidence supports this, and it is nonsensical
What about dose #20?

This slide does not account for changing facts on the ground. Omicron and prior immunity have drastically changed these numbers
PS these numbers we also wrong when they first put them forth, as we explained
medpagetoday.com/opinion/second…
PS these numbers we also wrong when they first put them forth, as we explained
medpagetoday.com/opinion/second…

Denmark is limiting vaccination to kids and young people.
US CDC has lost perspective, they are out of touch with data, the American people, and common sense
US CDC has lost perspective, they are out of touch with data, the American people, and common sense

• • •
Missing some Tweet in this thread? You can try to
force a refresh