*Advanced bedside monitoring in Resp failure*. Opening by Luigi Camporota to a room full of ventilation geeks from Paraguay, Australia, and all across Europe 😜 #LIVES2022
Starting with Luigi on the principles of why we ventilate , and linking with Driving Pressure to ensure lung protection (rather than TV)
1. Oesophageal pressure pubmed.ncbi.nlm.nih.gov/19001507/ but even if no oesophageal ballon 2. Bedside monitoring by clinician of Resp drive and asynchrony (E.g., breath stacking) is useful since high drive ~ VILI #LIVES2022
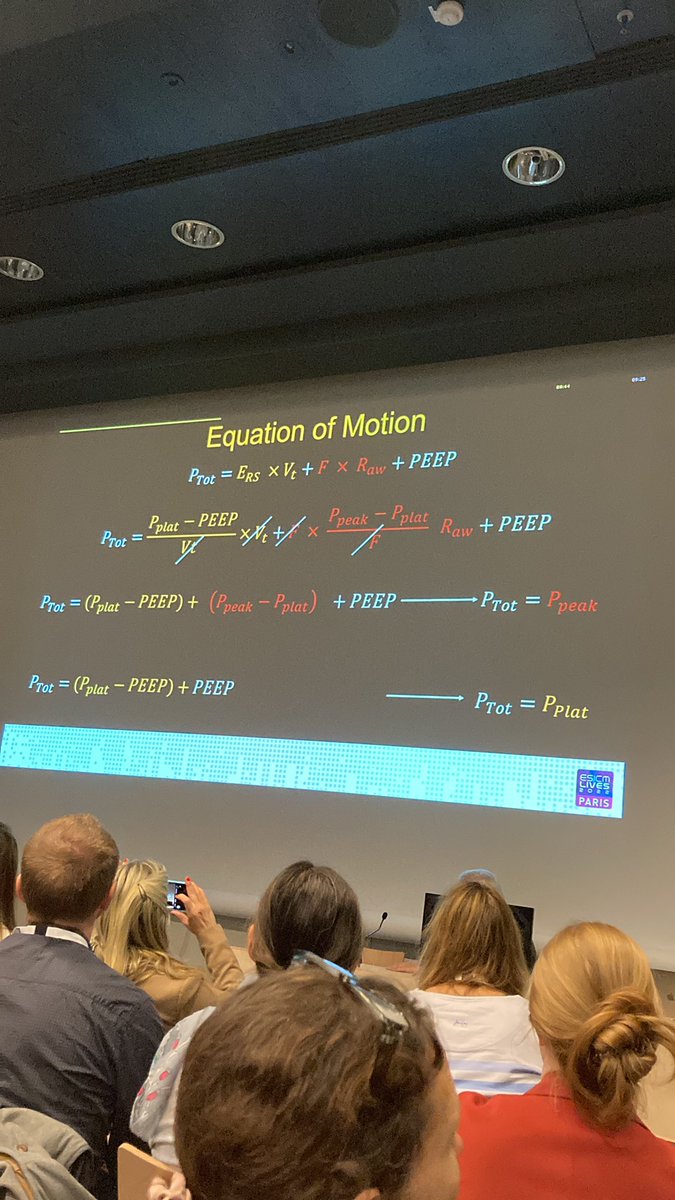
What I love about this is that it’s part of “your clinical examination and assessment”. *Respiratory Mechanics* - why do we assess ? Because we need to minimise VILI, understand the disease severity and process, evaluate response. And of course “equation of motion”.
P(tot) = elastic components + resistive components + PEEP. Effectively if there’s “movement”, Ptot = Ppeak. And if no movement, Ptot=Pplat 
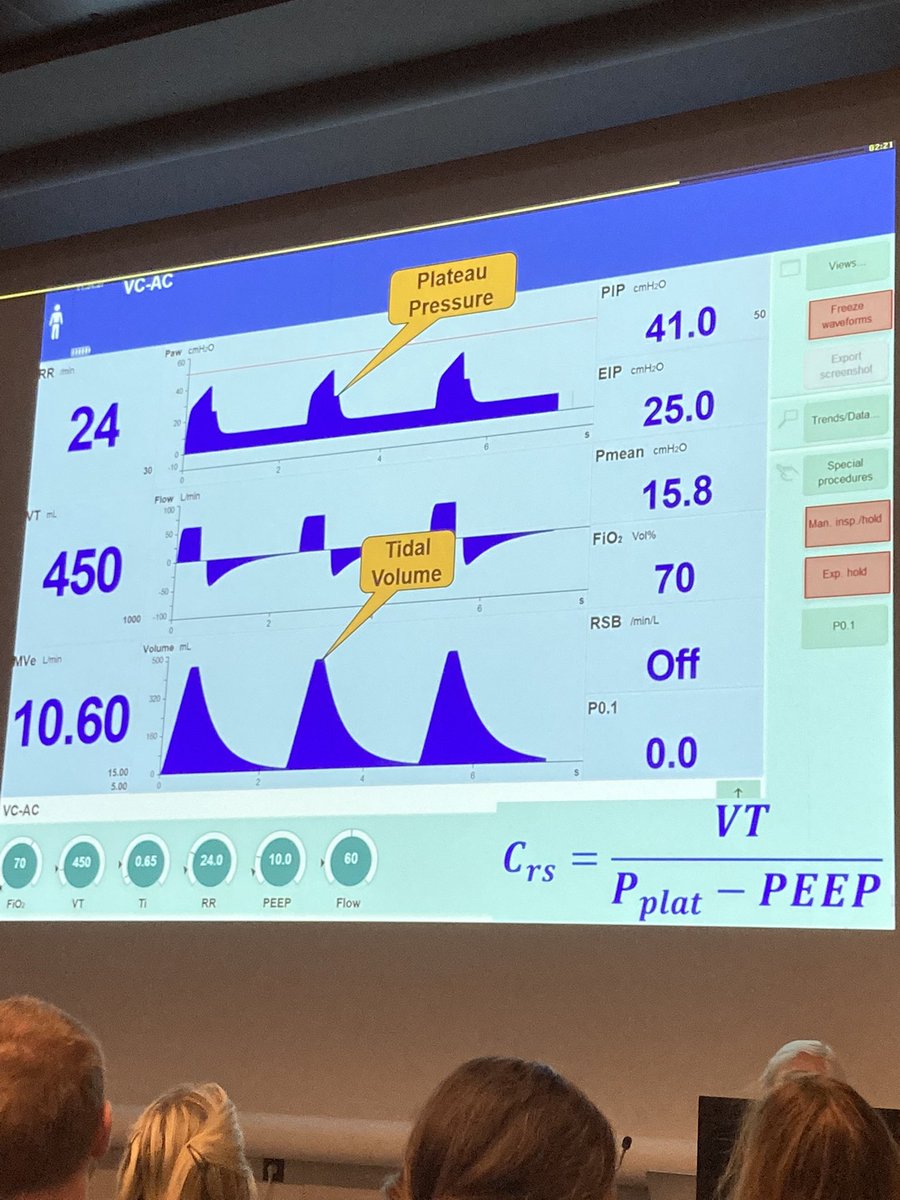
Pip vs Pleatau. If you change flow (in VC mode), you change PIP but not Pplateau. Now Compliance -> Crs = TV/(Pplat-PEEP) for this example 450/(40-25) = 450/15
But bear in mind intrinsic PEEP. (Either visually determines that expiratory flow returns to 0 or measure exp hold ). Now *low flow PV loop*. Demonstrating that PV loop takes into account airway opening pressure. See pic for demonstration
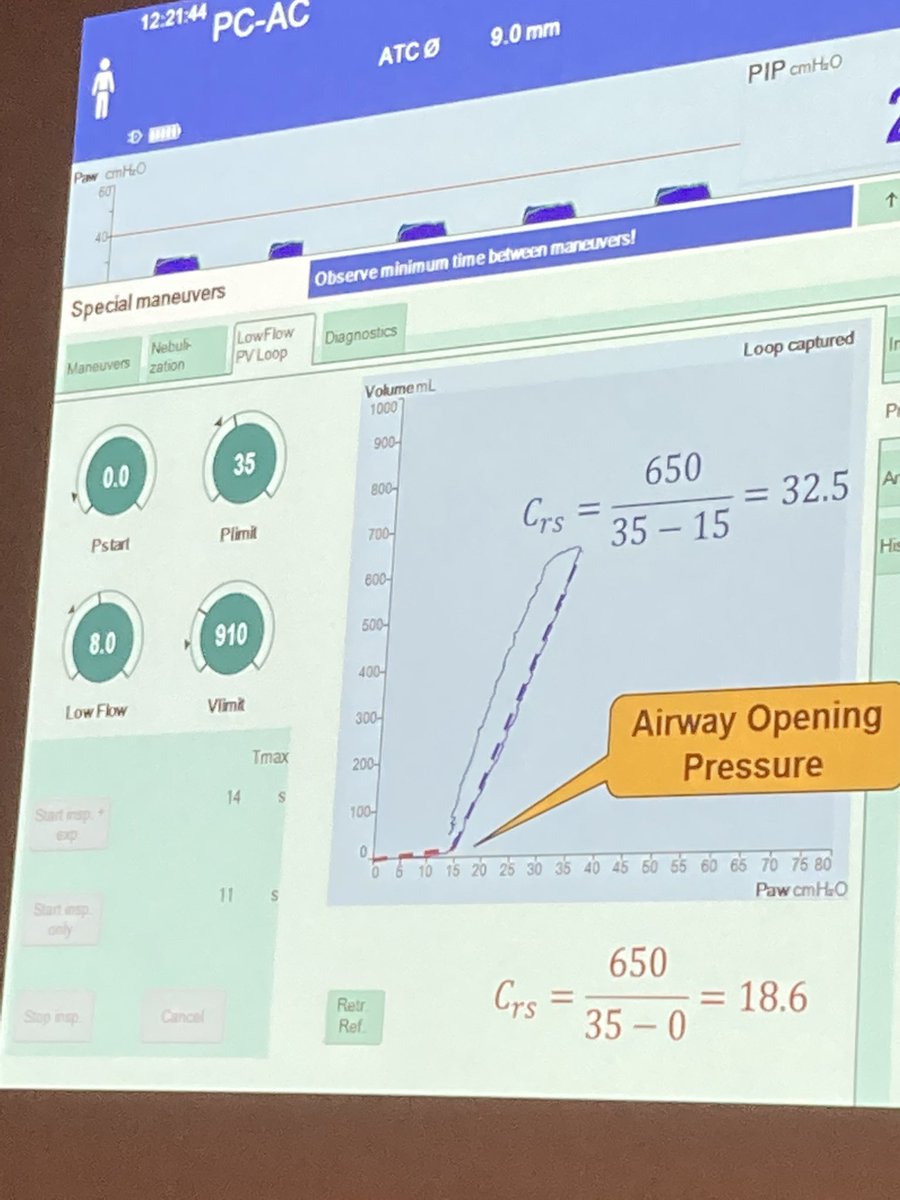
PV loop - standard is if patient is passive. But not necessarily need a muscle relaxant -> manoeuvre can be short and if patient is not making effort then it’s sufficient. #LIVES2022 #ventilation #CriticalCare
• • •
Missing some Tweet in this thread? You can try to
force a refresh