Antegrade Approach for #CTO Lesions #Cardiotwitter
Method A..Antegrade wire Escaltation ;
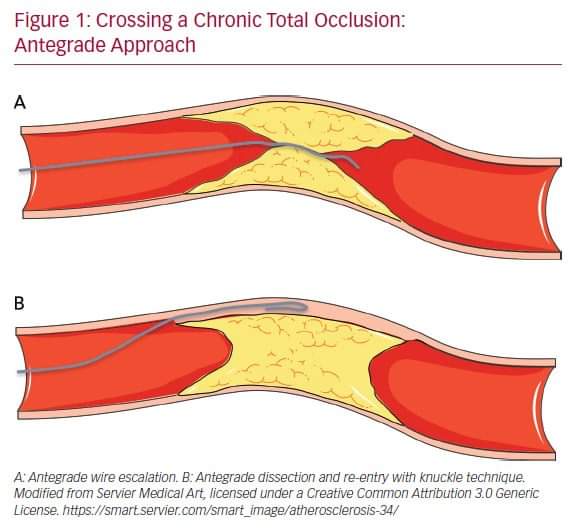
It consists of advancing various guidewires in antegrade direction to cross CTO while remaining within true lumen of vessel (True to True )
@mmamas1973
@mirvatalasnag
@Hragy
@PCRonline
Method A..Antegrade wire Escaltation ;
It consists of advancing various guidewires in antegrade direction to cross CTO while remaining within true lumen of vessel (True to True )
@mmamas1973
@mirvatalasnag
@Hragy
@PCRonline
#crossing proximal cap.
Wire escaltation
Wire Gear 1
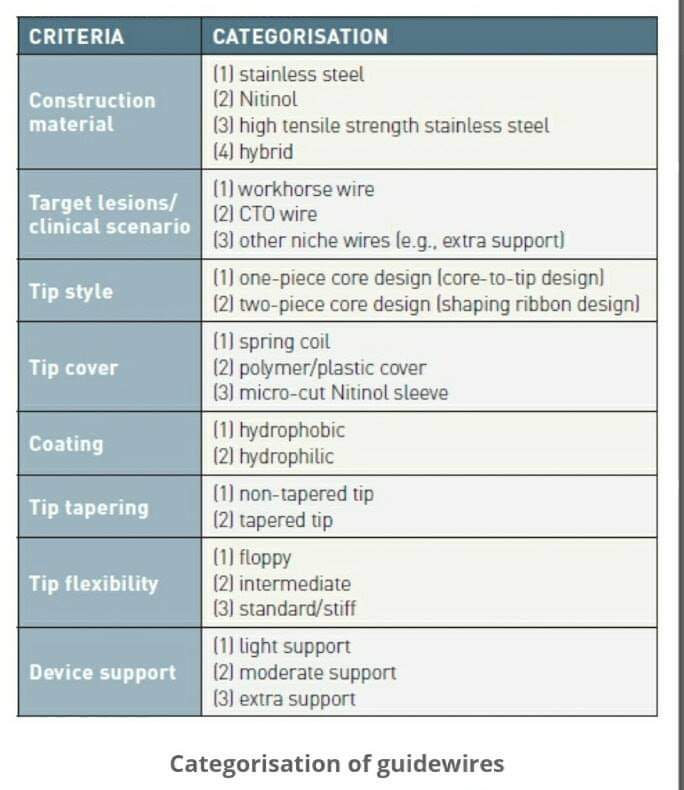
For proximal cap penetration, tapered polymer GW with low-penetration power soft-tip (Fielder family guidewires; Ashai Intecc), allowing advancement along visible or invisible microchannels, are the first choice
Wire escaltation
Wire Gear 1
For proximal cap penetration, tapered polymer GW with low-penetration power soft-tip (Fielder family guidewires; Ashai Intecc), allowing advancement along visible or invisible microchannels, are the first choice
Wire Gear 2
~If the operator encounters difficulties in crossing the lesion, they can switch to GW with greater penetration force. When proximal cap is blunt, GW with intermediate penetration force (Gaia 2nd–3rd [Ashai Intecc] or Pilot 200 [Abbott Vascular]) are used.
~If the operator encounters difficulties in crossing the lesion, they can switch to GW with greater penetration force. When proximal cap is blunt, GW with intermediate penetration force (Gaia 2nd–3rd [Ashai Intecc] or Pilot 200 [Abbott Vascular]) are used.
Wire Gear 3.
~If ineffective, GW with high penetration force (Conquest Pro 9-12 [Ashai Intecc] or Hornet 10-14 [Boston Scientific]) are used. In addition, use of a microcatheter, placed near lesion, may be helpful to increase support and penetration power of the guidewire
~If ineffective, GW with high penetration force (Conquest Pro 9-12 [Ashai Intecc] or Hornet 10-14 [Boston Scientific]) are used. In addition, use of a microcatheter, placed near lesion, may be helpful to increase support and penetration power of the guidewire
De escaltating wires ;
Once the proximal cap has been penetrated, de-escalation to less penetrating GW can be carried out
(quick and precise changing of GW is made easier by presence of a microcatheter)
Once the proximal cap has been penetrated, de-escalation to less penetrating GW can be carried out
(quick and precise changing of GW is made easier by presence of a microcatheter)
2.Entry Techniques for Proximal cap ..
There are several methods for advancing the GW in true-to-true lumen technique.
•Sliding
•Drilling
•Push & Torque
There are several methods for advancing the GW in true-to-true lumen technique.
•Sliding
•Drilling
•Push & Torque
•Sliding technique
~In the sliding technique, using tapered polymer guidewires with soft tips, slight rotational movements and cautious advances are used to cross the lesion.
~In the sliding technique, using tapered polymer guidewires with soft tips, slight rotational movements and cautious advances are used to cross the lesion.
Drilling technique, performed when there are harder caps, consists of advancing the GW, making rotational movements less than 90°. In presence of more calcified lesions operator may proceed with penetration technique in which stiff GW are pushed without rotational movements
~Push & Torque technique
In this technique operator advances & rotates GW until hardest portion of plaque is reached & then redirects it to a softer part. Once lesion is crossed, in order to understand where GW is located, it is necessary to perform contralateral injection
In this technique operator advances & rotates GW until hardest portion of plaque is reached & then redirects it to a softer part. Once lesion is crossed, in order to understand where GW is located, it is necessary to perform contralateral injection
If during wiring escalation technique, GW accidentally reaches subintimal space, it is possible to proceed with dissection & re-entry technique. Alternatively GW can be left in subintimal space as reference & 2nd GW advanced through plaque (parallel guidewire technique
Method B...#Dissection Sub intimal re entry techniques ;
~STAR techniques
~Stingry Balloon technique
~LAST techniques
~STAR techniques
~Stingry Balloon technique
~LAST techniques
1 STAR Technique
Here knuckled GW advanced in subintimal space
Subsequent re-entry into distal lumen is unpredictable & uncontrollable. This implies that stent is implanted in long subintimal tract with higher risk of branch occlusion & vessel restenosis.
Here knuckled GW advanced in subintimal space
Subsequent re-entry into distal lumen is unpredictable & uncontrollable. This implies that stent is implanted in long subintimal tract with higher risk of branch occlusion & vessel restenosis.
2..Controlled Dissection & Re entry techniques through Stingray balloon system .
1.Stingray balloon is placed in subintimal space beyond distal cap of CTO
2.A stiff wire is passed through lumen of stingray balloon into distal vessels
1.Stingray balloon is placed in subintimal space beyond distal cap of CTO
2.A stiff wire is passed through lumen of stingray balloon into distal vessels
3.Limited Dissection & Re entry (LAST Technique )
Limited dissection and re-entry techniques can lead to a lower risk of restenosis and target vessel revascularization.
Limited dissection and re-entry techniques can lead to a lower risk of restenosis and target vessel revascularization.
• • •
Missing some Tweet in this thread? You can try to
force a refresh