Hey #GIOnc #Radonc friends! Let’s talk definitive CRT for locally advanced esophagus cancer! Looks like we now have at least 5 RCTs exploring dose escalation… and the standard remains 50 Gy! Let’s review!! 🧵🧵🧵1/ 

RTOG 8501 established the standard care of 50.4 Gy + concurrent chemotherapy for patients with inoperable, locally advanced esophagus cancer
Nearly 90% were SCC.
🔵Long-term disease control/survival was achieved in approximately 25% of patients. 0% with RT alone!!! 2/
Nearly 90% were SCC.
🔵Long-term disease control/survival was achieved in approximately 25% of patients. 0% with RT alone!!! 2/

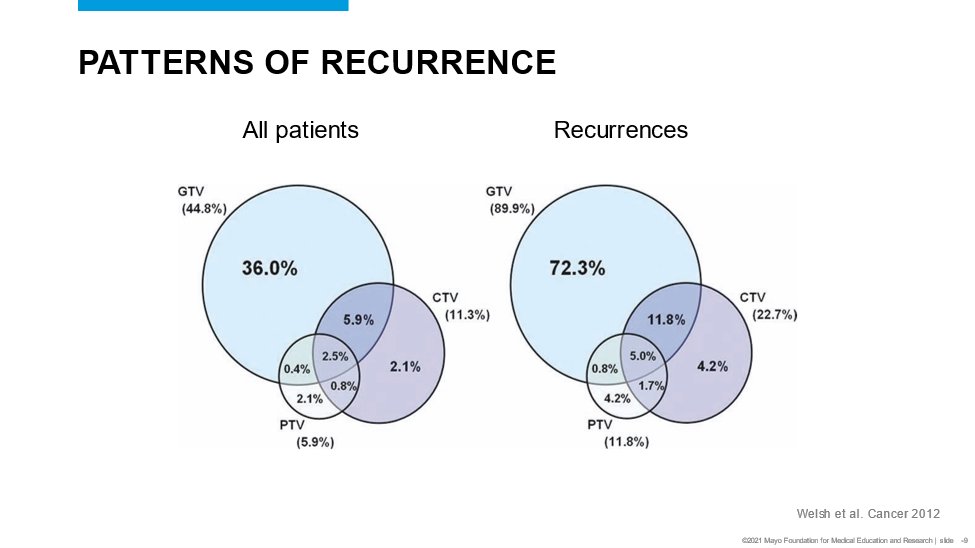
However, local progression after 50.4 Gy + chemo occurs in approximately 50% of patients AND the vast majority occur at sites of initial gross disease. Hence the question: Would increasing RT dose improve outcomes??? 3/

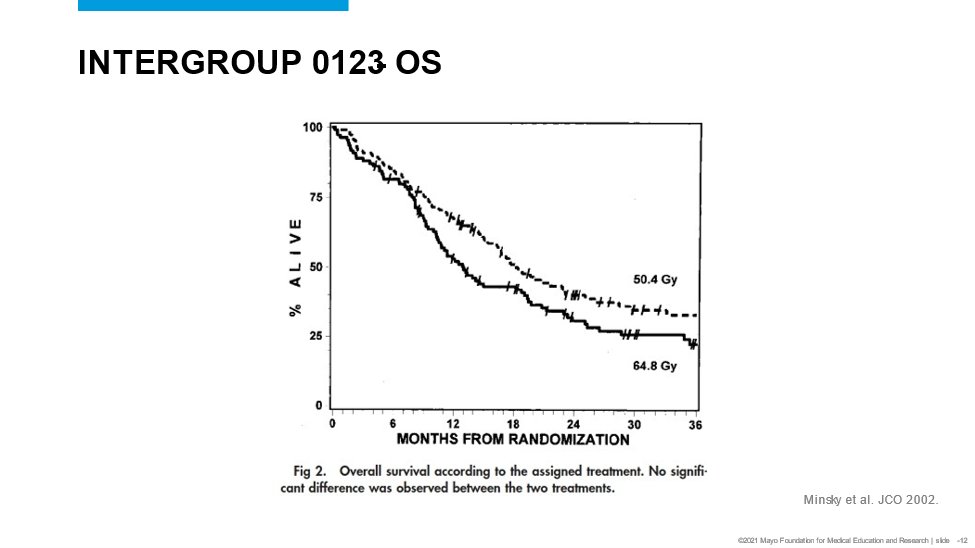
Intergroup 0123 first explored this question
50.4 vs. 64.8 Gy (1.8 Gy fxs) + cisplatin/5-FU
Key outcomes:
🔵Dose escalation DID NOT improve OS or local progression.
🔵50.4 Gy remained the standard 4/
50.4 vs. 64.8 Gy (1.8 Gy fxs) + cisplatin/5-FU
Key outcomes:
🔵Dose escalation DID NOT improve OS or local progression.
🔵50.4 Gy remained the standard 4/



Next up (almost 20 years later) in the IMRT “era”
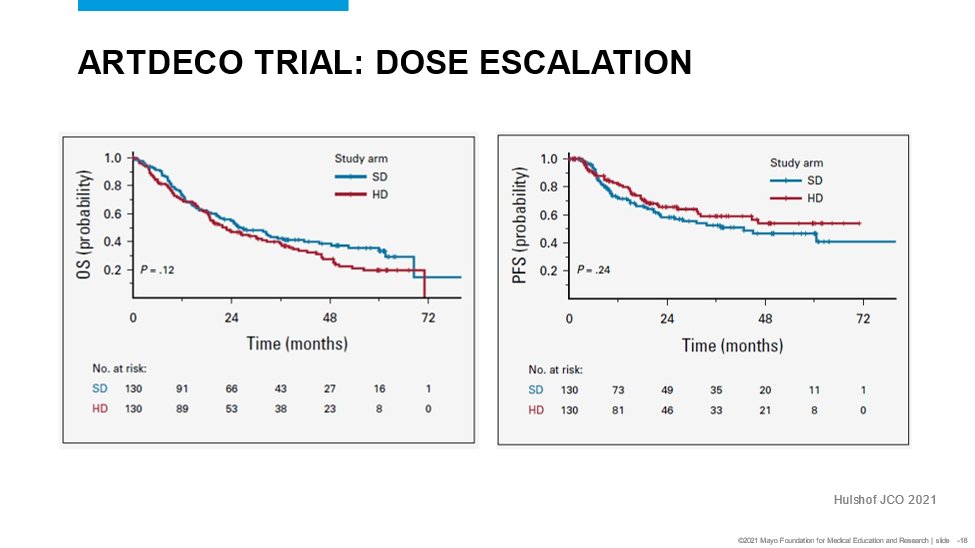
ARTDECO Trial
50.4 vs. 61.6 each in 28 fractions with carbo/taxol
SAME STORY!
Dose escalation DID NOT improve OS, PFS, or locoregional PFS 5/
ARTDECO Trial
50.4 vs. 61.6 each in 28 fractions with carbo/taxol
SAME STORY!
Dose escalation DID NOT improve OS, PFS, or locoregional PFS 5/


🔥🔥Hot of the press!!!
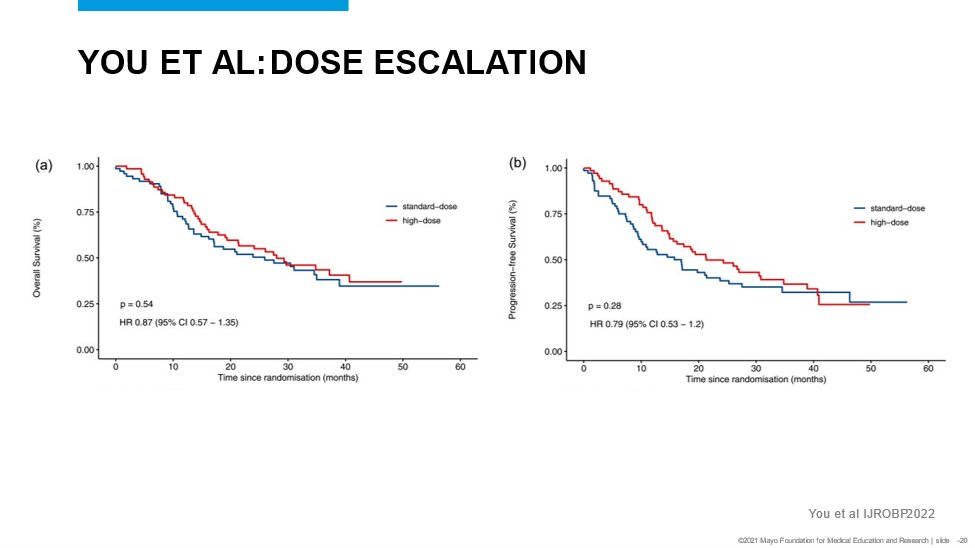
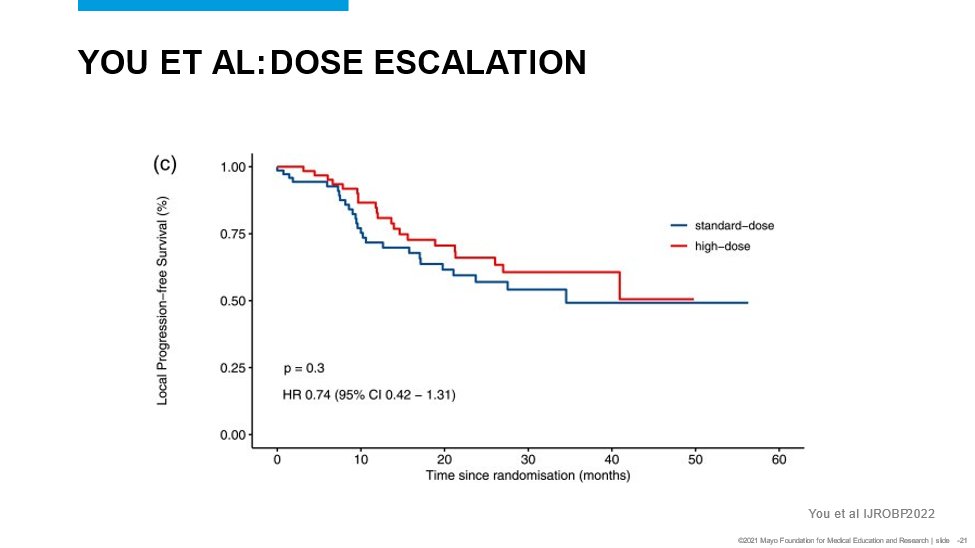
You et al @IJROBP
Locally advanced, inoperable, thoracic esophagus SCC.
Randomized: 50.4 vs. 59.4 Gy with carbo/taxol
You guessed it: no improvement in OS, PFS, or local control with 59.4 Gy compared with 50.4 Gy 6/
You et al @IJROBP
Locally advanced, inoperable, thoracic esophagus SCC.
Randomized: 50.4 vs. 59.4 Gy with carbo/taxol
You guessed it: no improvement in OS, PFS, or local control with 59.4 Gy compared with 50.4 Gy 6/

There are at least 2 others reported:
PRODIGE 26: 50 Gy vs. 66 Gy with concurrent FOLFOX sciencedirect.com/science/articl…
Xu et al: 50 vs 60 Gy concurrent docetaxel/cisplatin.
Neither study showed improved OS, PFS, or local control with 60/66 Gy when compared to 50. 7/
PRODIGE 26: 50 Gy vs. 66 Gy with concurrent FOLFOX sciencedirect.com/science/articl…
Xu et al: 50 vs 60 Gy concurrent docetaxel/cisplatin.
Neither study showed improved OS, PFS, or local control with 60/66 Gy when compared to 50. 7/



Conclusion: 50 Gy is the SOC!!!
I think improvements are going to come through incorporating novel radiosensitizers and/or maintenance systemic tx (ie. ICI). Not RT dose...
Hey med onc friends! Lets collaborate!!! 8/8
I think improvements are going to come through incorporating novel radiosensitizers and/or maintenance systemic tx (ie. ICI). Not RT dose...
Hey med onc friends! Lets collaborate!!! 8/8
• • •
Missing some Tweet in this thread? You can try to
force a refresh