
What should you call that elevated troponin?
This is NOT taught well and impacts more than you think.
Understand it in 2 minutes:
This is NOT taught well and impacts more than you think.
Understand it in 2 minutes:
The problem?
💙 Most don't understand how to interpret troponins
💙 Most don't understand the actual definition of an infarction
💙 Proper diagnosis (& documentation) ➡️ impacts clinical decisions and quality metrics
Let's dig in ⤵️
💙 Most don't understand how to interpret troponins
💙 Most don't understand the actual definition of an infarction
💙 Proper diagnosis (& documentation) ➡️ impacts clinical decisions and quality metrics
Let's dig in ⤵️
First, pay close attention to the three I-words:
1️⃣ Injury
2️⃣ Ischemia
3️⃣ Infarction
They have three distinct meanings and easy to get them mixed up.
1️⃣ Injury
2️⃣ Ischemia
3️⃣ Infarction
They have three distinct meanings and easy to get them mixed up.
Two things must be present for an acute Myocardial INFARCTION
1️⃣ Acute myocardial INJURY
2️⃣ ISCHEMIC Signs OR symptoms
(notice the *OR* here)
Let's break those down.
First, myocardial injury...
1️⃣ Acute myocardial INJURY
2️⃣ ISCHEMIC Signs OR symptoms
(notice the *OR* here)
Let's break those down.
First, myocardial injury...
1 / What is INJURY?
A fluctuation of troponins by 20%. Whether this be:
💙 A rise of 20% (with at least one elevated or
💙 A fall of 20% if initial was elevated
What if elevated but does not change by 20%? Will answer this later.
Next, ischemia...
A fluctuation of troponins by 20%. Whether this be:
💙 A rise of 20% (with at least one elevated or
💙 A fall of 20% if initial was elevated
What if elevated but does not change by 20%? Will answer this later.
Next, ischemia...
2 / What are ISCHEMIC Signs & symptoms?
Symptoms
💙 Angina
💙 Anginal Equivalents (SOB, diaphoresis, nausea, lightheadedness)
💙 Syncope
💙 Flash pulmonary edema
💙 Palpations
💙 Cardiac arrest
and signs?...
Symptoms
💙 Angina
💙 Anginal Equivalents (SOB, diaphoresis, nausea, lightheadedness)
💙 Syncope
💙 Flash pulmonary edema
💙 Palpations
💙 Cardiac arrest
and signs?...
Signs
💙 ST elevation or depression
💙 New flipped T wave
💙 New LBBB
💙 New pathological Q waves
💙 NM stress with new loss of viable myocardium (NOT scar)
💙 New ventricular wall motion abnormality
💙 Identification of coronary thrombus on LHC or autopsy
💙 ST elevation or depression
💙 New flipped T wave
💙 New LBBB
💙 New pathological Q waves
💙 NM stress with new loss of viable myocardium (NOT scar)
💙 New ventricular wall motion abnormality
💙 Identification of coronary thrombus on LHC or autopsy
3 / What are the types of INFARCTions?
Type 1 (STEMI vs NSTEMI)
💙 Acute coronary artery occlusion due to plaque disruption
💙 Treatment ➡️ dissolve clot / open blockage
(Reminder: Must have Injury + Ischemic signs or symptoms)
Type 1 (STEMI vs NSTEMI)
💙 Acute coronary artery occlusion due to plaque disruption
💙 Treatment ➡️ dissolve clot / open blockage
(Reminder: Must have Injury + Ischemic signs or symptoms)

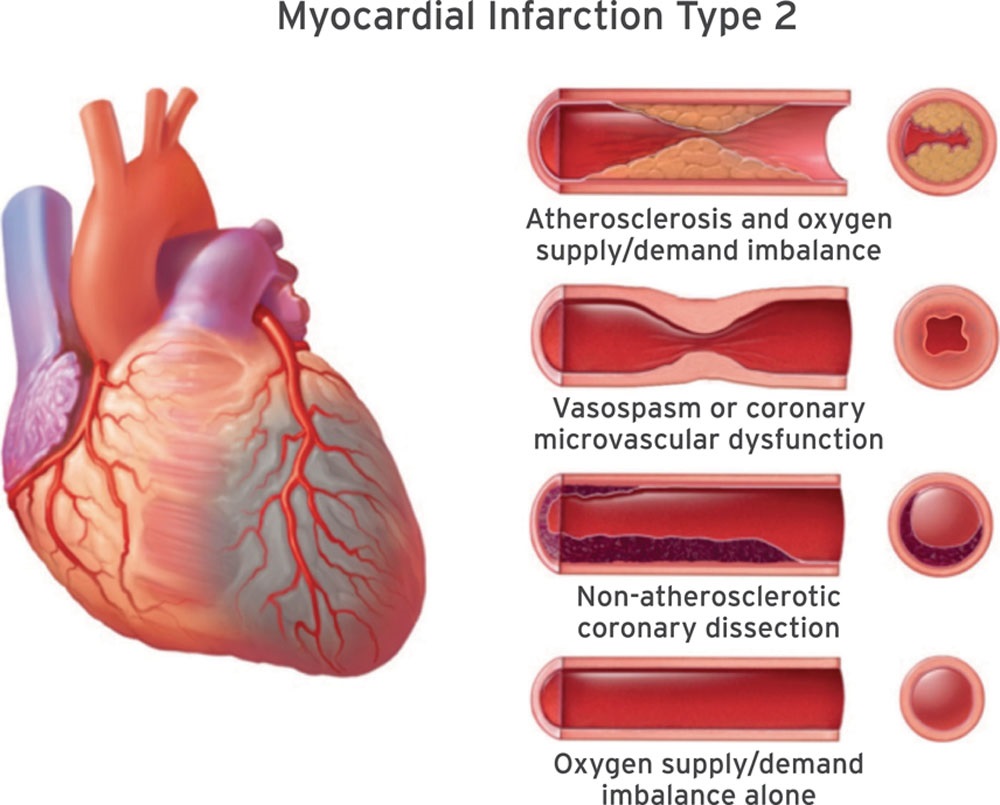
Type 2 (NSTEMI)
💙 Imbalance between myocardial oxygen supply and/or demand results in INFARCTion
💙 Treatment ➡️ relieve demand / non-CAD factors
(Reminder: Must have Injury + Ischemic signs or symptoms)
💙 Imbalance between myocardial oxygen supply and/or demand results in INFARCTion
💙 Treatment ➡️ relieve demand / non-CAD factors
(Reminder: Must have Injury + Ischemic signs or symptoms)
Other types of infarctions:
Type 3 = Sudden death without biomarkers
Type 4a = PCI related AMI
Type 4b = Due to stent thrombosis
Type 4c = Stent re-stenosis
TYpe 5 = CABG related.
Won't go into detail about these.
Type 3 = Sudden death without biomarkers
Type 4a = PCI related AMI
Type 4b = Due to stent thrombosis
Type 4c = Stent re-stenosis
TYpe 5 = CABG related.
Won't go into detail about these.
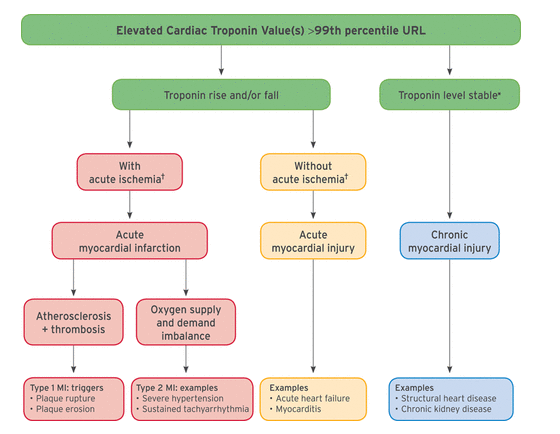
4 / What about elevated troponins alone?
That is myocardial INJURY w/o ischemia (thus not infarction)
💙 20% rise / fall? = Acute Injury
Ex: Acute CHF, myocarditis, etc.
💙 No 20% rise / fall? = Chronic injury
Ex: CKD, structural heart disease, etc.
Your "troponin leaks"
That is myocardial INJURY w/o ischemia (thus not infarction)
💙 20% rise / fall? = Acute Injury
Ex: Acute CHF, myocarditis, etc.
💙 No 20% rise / fall? = Chronic injury
Ex: CKD, structural heart disease, etc.
Your "troponin leaks"
5 / What is Demand Ischemia?!
This DOES NOT exist in the 4th universal definition of MI.
but it does in coding.
Guidance is unclear & conflicting.
Use this if:
💙 Have a setting of supply / demand mismatch
💙 But have ischemia WITHOUT injury (but not both bc then = T2 NSTEMI)
This DOES NOT exist in the 4th universal definition of MI.
but it does in coding.
Guidance is unclear & conflicting.
Use this if:
💙 Have a setting of supply / demand mismatch
💙 But have ischemia WITHOUT injury (but not both bc then = T2 NSTEMI)
In summary:
1️⃣ Myocardial Injury = 20% change of elevated troponins
2️⃣ Infarct = Injury + Ischeimic signs *OR* symptoms
3️⃣ Troponemia, troponin leak, troponitis, & Elevated troponin are not diagnoses.
4️⃣ Demand ischemia = ischemia without injury
1️⃣ Myocardial Injury = 20% change of elevated troponins
2️⃣ Infarct = Injury + Ischeimic signs *OR* symptoms
3️⃣ Troponemia, troponin leak, troponitis, & Elevated troponin are not diagnoses.
4️⃣ Demand ischemia = ischemia without injury
This all has downstream impacts too nuanced for a Twitter thread. Subscribe to my newsletter for a deeper dive (link in bio).
If you enjoyed this thread:
1. Follow me @Dr_Oubre for more of these
2. RT the tweet below to share this thread with your audience
If you enjoyed this thread:
1. Follow me @Dr_Oubre for more of these
2. RT the tweet below to share this thread with your audience
https://twitter.com/Dr_Oubre/status/1593974704376754181
Subscribers get discounts on my future ebooks, courses, etc
Sign up for my free newsletter (link in Bio).
Won’t spam you. Easy to unsubscribe.
Sign up for my free newsletter (link in Bio).
Won’t spam you. Easy to unsubscribe.
• • •
Missing some Tweet in this thread? You can try to
force a refresh





