An educational 🧵on looking beyond just response rates in a single arm Phase II trial and learning from the story of cilta-cel in CARTIFAN.
This trial has many golden lessons on critical appraisal/global disparity, and this🧵is for trainees/fellows/pharmacists
#mmsm
1/
This trial has many golden lessons on critical appraisal/global disparity, and this🧵is for trainees/fellows/pharmacists
#mmsm
1/
Cilta-cel is a chimeric antigen receptor cell therapy that is very promising, and targets BCMA on myeloma cells.
We have data from other trials (CARTITUDE-1), that cilta-cel is associated with a very high-response rate in those who are able to receive it.
We have data from other trials (CARTITUDE-1), that cilta-cel is associated with a very high-response rate in those who are able to receive it.
In this trial, patients from China with relapsed/refractory MM enrolled with the intent to give cilta-cel.
The conclusion says that cilta-cel had a favorable risk-benefit profile and that response rate is 89.6%
Lets dig in a little.
The conclusion says that cilta-cel had a favorable risk-benefit profile and that response rate is 89.6%
Lets dig in a little.
When we say response rate is 89.6%, what is the denominator? This is the KEY point.
A total of 64 patients were enrolled, yet only 48 got cilta-cel, of which 43 responded
The denominator should be the number of patients that were enrolled, reflecting "intent to treat".
A total of 64 patients were enrolled, yet only 48 got cilta-cel, of which 43 responded
The denominator should be the number of patients that were enrolled, reflecting "intent to treat".
Significant attrition between enrollment and receipt of product is a sign of patients with most aggressive disease biology (those who need product the most) being filtered out.
This is a key real world limitation!
This is a key real world limitation!
Reported response rate 43/48=89.6%
Intent to treat response: 43/64=67.2%
Now, that is a HUGE difference.
What happened to all of these other patients?
More on that.
Intent to treat response: 43/64=67.2%
Now, that is a HUGE difference.
What happened to all of these other patients?
More on that.
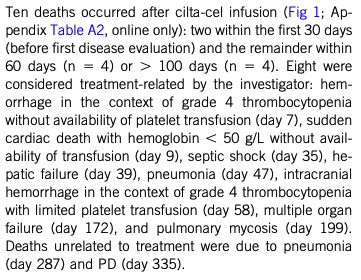
And lets talk a little bit about mortality rate.
How meaningful is a response if you die from a treatment side effect within a few weeks/months of the treatment?
Again, focusing exclusively on response rates hides important things such as DEATH!
How meaningful is a response if you die from a treatment side effect within a few weeks/months of the treatment?
Again, focusing exclusively on response rates hides important things such as DEATH!
So, 10 patients died after CART! Now 10/48 patients dying so soon (median f/up=18 months) after CART is a really toxic intervention!
Such a high death rate was not seen in the initial cilta-cel study. So what happened?
Such a high death rate was not seen in the initial cilta-cel study. So what happened?
This study raises important questions on access/infrastructure.
I would argue deaths related to lack of transfusions were preventable. It truly is tragic that a 465,000$ intervention can be given but resources for blood transfusions cannot be provided in same institutions.
I would argue deaths related to lack of transfusions were preventable. It truly is tragic that a 465,000$ intervention can be given but resources for blood transfusions cannot be provided in same institutions.
Other troubling infection related signal also maybe preventable?
Five patients had HBV reactivation, 3 had new HBV infection. Remember, the sample size is only 48.
Was the one hepatic failure death related? Also troubling/needs attention. HBV surveil/ppx could have prevented.
Five patients had HBV reactivation, 3 had new HBV infection. Remember, the sample size is only 48.
Was the one hepatic failure death related? Also troubling/needs attention. HBV surveil/ppx could have prevented.
Toci was given liberally for CRS (91% receipt), hence it is puzzling that less expensive/more commonplace interventions were not available.
Sadly, it appears better antimicrobial ppx and blood transfusions could have prevented at least some of these deaths.
Sadly, it appears better antimicrobial ppx and blood transfusions could have prevented at least some of these deaths.
We take many of these things for granted in the US, this is a sobering reminder of disparities that exist globally
Highlights needs to reinforce/prioritize basic infrastructure needs prior to introducing sexy new technology such as CART
Highlights needs to reinforce/prioritize basic infrastructure needs prior to introducing sexy new technology such as CART
Furthermore, cilta-cel was given to these patients prior to other more established agents such as daratumumab. Only 31% exposed to daratumumab.
Given "preventable" death and lack of exposure to proven agents, especially unfortunate.
Given "preventable" death and lack of exposure to proven agents, especially unfortunate.
The purpose of this thread is to raise awareness about critical analysis of trials (look beyond response rates!), reinforce intent to treat analysis, ponder over global infrastructure disparities, and contextualize response rates with overall death rates from an intervention.
Hopefully this thread was helpful. Happy Thanksgiving 🦃
I am not the first to highlight this- I credit @AaronGoodman33 , @HadidiSamer ,@rajshekharucms and @HiraSMian for drawing attention to these things and helping refine our collective critical analysis skills.
END.
I am not the first to highlight this- I credit @AaronGoodman33 , @HadidiSamer ,@rajshekharucms and @HiraSMian for drawing attention to these things and helping refine our collective critical analysis skills.
END.
• • •
Missing some Tweet in this thread? You can try to
force a refresh