
This is a really brilliant representation of Denmark’s RSV admissions data. It shows what I’ve been trying to explain for a while now. Delaying RSV exposure is *good*. The babies born in the 20/21 “gap year” experienced a net *benefit* by dodging RSV en masse as infants. 1/ 
https://twitter.com/barclaybenedict/status/1597172291447971840

Not exposing infants that season resulted in a net decrease of total RSV hospitalizations for that cohort over time. This is consistent with what we’ve known for decades which is that RSV is most dangerous for 0-12 month olds and there’s a net benefit to delaying exposure. 2/
In other words:
- no immunity debt — no increased risk of hosp from delayed exposure
- some immunity gap — many went on to be hospitalized in 21/22 at 12-24 months and 22/23 at 24-36 months, but not all
- we see evidence of some immunity *CREDIT* — averted hospitalizations
3/
- no immunity debt — no increased risk of hosp from delayed exposure
- some immunity gap — many went on to be hospitalized in 21/22 at 12-24 months and 22/23 at 24-36 months, but not all
- we see evidence of some immunity *CREDIT* — averted hospitalizations
3/

So there you have it. There’s no benefit to exposing infants to RSV. The cohort of kids that were infants the year that RSV stopped circulating went on to have a lower total number RSV hospitalizations. We didn’t just delay the inevitable. We *prevented* hospitalizations. 4/

And now with that in mind, how do we explain why the 21/22 and 22/23 babies have been hospitalized for RSV in their first RSV season as infants (0-12 months) at much higher rates than the cohorts that came before them? Neither immunity debt nor immunity gap can explain this. 5/

Any MD w an ounce of integrity would say the #1 suspect for increased susceptibility of infants to severe RSV in the pandemic era is covid. Whether it’s immune dysfunction or lung dysfunction or something else, SARS2 is the most likely reason that these babies are different. /6

Alright so I’m circling back to this because it seems that some people still don’t understand what this data shows.
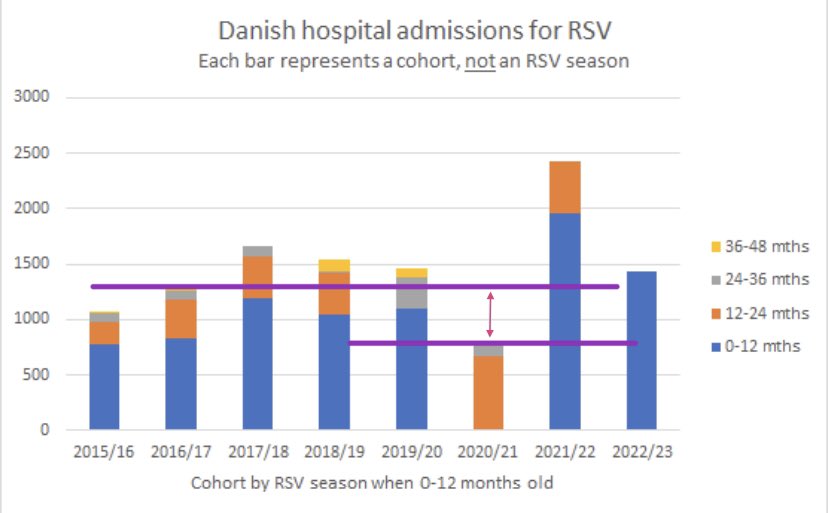
The X axis of this graph is *cohorts of babies*, not years. The cohorts are divided up based on first RSV season as infants.
The X axis of this graph is *cohorts of babies*, not years. The cohorts are divided up based on first RSV season as infants.


The bars show the ages at which the kids in each cohort ended up in the hospital with RSV. The years they were admitted are NOT on the graph! This is cumulative RSV admissions by cohort + their age on admission.
The unexposed gap year babies have the *lowest* cumulative total.
The unexposed gap year babies have the *lowest* cumulative total.

Here I’ve added the years they were admitted to the graph. @jmcrookston also did a good job breaking it down in his tweet.
https://twitter.com/jmcrookston/status/1597328458082058241

Ok so here’s the smoking gun: the double cohort
So the “immunity gap” or “double cohort” effect stipulates that the increase in admissions during the rebound RSV epidemic is a game of catch up where the gap year 20/21 cohort and the 21/22 cohort are all exposed at the same time.
So the “immunity gap” or “double cohort” effect stipulates that the increase in admissions during the rebound RSV epidemic is a game of catch up where the gap year 20/21 cohort and the 21/22 cohort are all exposed at the same time.
Look again. The 2020/21 cohort and the 2021/22 cohort were exposed to the same 2 RSV seasons: 2021/22 and this year 2022/23. If this was just a game of catch up, of inevitability of RSV admissions, then these 2 cohorts should have the same cumulative total. They don’t.

Not only do the 20/21 cohort and 21/22 cohort not have the same cumulative total despite being exposed to the same 2 RSV seasons, what we see is a protective effect of the gap year for the 20/21 kids (lower total RSV admissions) and *excess RSV admissions* for the 21/22 cohort!!

Basically, not exposing the 20/21 cohort to RSV as infants prevented many hospitalizations. Not being exposed to RSV early was a net positive for these kids. And we see that the subsequent cohorts (21/22 and 22/23 babies) have an increased susceptibility to severe RSV.


In case it’s still not clear, @BarclayBenedict provided a second way to visualize the cumulative RSV admissions data by cohort here, that I also annotated for you to highlight the prepandemic average vs the 20/21 gap year kids and the 21/22 + 22/23 babies.
https://twitter.com/BarclayBenedict/status/1597330011387990016

Again, we can clearly see that there are less cumulative RSV admissions for the gap year kids (getting rid of RSV during their infancy prevented many of them from being hospitalized!) and excess RSV admissions for kids exposed to RSV in infancy in the pandemic era.

So what’s not behind the rise in RSV hospitalizations (and the peds crisis):
- immunity debt✖️
nope, non-exposure in infancy was an advantage
- cohort effect alone✖️
total hospitalizations are lower for the non-exposed cohort and higher than expected for the subsequent cohorts
- immunity debt✖️
nope, non-exposure in infancy was an advantage
- cohort effect alone✖️
total hospitalizations are lower for the non-exposed cohort and higher than expected for the subsequent cohorts
So what is behind the rise in RSV hospitalizations (and the peds crisis)?
Increased susceptibility to severe RSV for kids born in 2021/2022 and the current 2022/23 infant cohort.
Increased susceptibility to severe RSV for kids born in 2021/2022 and the current 2022/23 infant cohort.

I don’t know exactly what made these babies more susceptible to severe RSV infections but as I’ve pointed out before, we need to be looking at the role of covid infections in utero on outcomes in infancy. Don’t @ me w claims of “generational immunity debt”. Read this 🧵 instead:
https://twitter.com/jvipondmd/status/1597320873119477760
And then follow it up with this 🧵
There’s lots of evidence that covid + pregnancy = badness. And these studies were pre-vaccine (sorry antivaxxers). We know now that in general the vaccines are good at lowering the odds of covid-related badness but are only partially protective.
There’s lots of evidence that covid + pregnancy = badness. And these studies were pre-vaccine (sorry antivaxxers). We know now that in general the vaccines are good at lowering the odds of covid-related badness but are only partially protective.
https://twitter.com/lisa_iannattone/status/1593827469882052610
Let me put it this way, if SARS2 was a new drug given in pregnancy and we saw these outcomes in infants in the years following its introduction, it would have been pulled from the shelves already. Normally, we would be quick on the trigger to protect pregnant women and infants.
But nothing about the current era is normal anymore is it?
Further reading. “Immunity debt” and “immunity gap” don’t explain the increased susceptibility of 45+ year olds to severe RSV either.👇🏻
https://twitter.com/barclaybenedict/status/1597252430625792000
And a thread on the 2 RSV waves in Denmark since the 1 missed RSV season 2 years ago. Compared to the rebound season in 2021/22 last year, there’s less RSV and more admissions per cases this year. Thank you for sharing all of this very informative data @BarclayBenedict.
https://twitter.com/barclaybenedict/status/1595814867822383106
• • •
Missing some Tweet in this thread? You can try to
force a refresh







