
Way back in April of this year, I received a kind invitation from @PaulPottingerMD to speak about Twitter at this year’s IDWeek.
1/x
1/x

Sounded like fun--plus I could learn from @KrutikaKuppalli and @Payal_Patel, so I readily accepted ...
... little imagining that shortly after IDWeek, this site would be embroiled in various controversies -- about which many others have already weighed in wisely!
2/x
... little imagining that shortly after IDWeek, this site would be embroiled in various controversies -- about which many others have already weighed in wisely!
2/x
But here's a condensed version of the talk, which explains why I'm sticking around (at least for now).
Let’s start with the (dreaded) “Learning Objectives”, which I’ve tried to enliven with pic of my pup.
3/x
Let’s start with the (dreaded) “Learning Objectives”, which I’ve tried to enliven with pic of my pup.
3/x

People who don’t use Twitter might be thinking along the same lines as Dr. Milton Packer. medpagetoday.com/opinion/revolu…
4/x
4/x
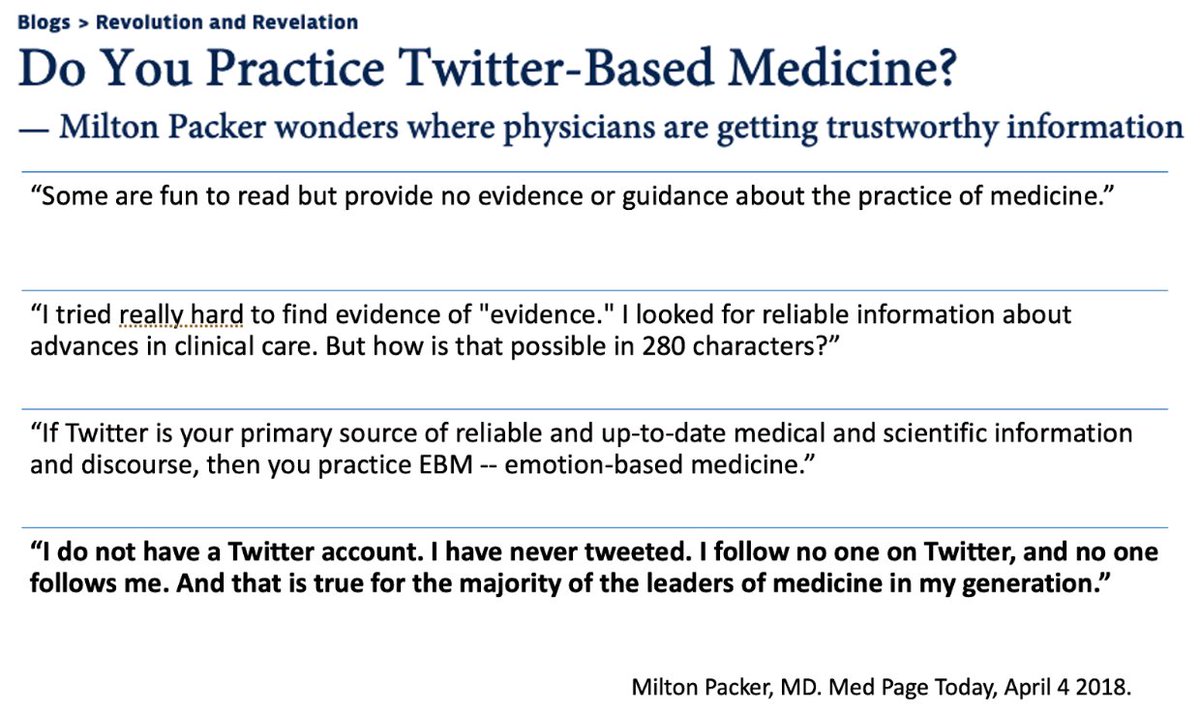
He makes several valid points, which I further summarize here.
(Stay tuned, the "Rules" come at the end of this thread.)
5/x
(Stay tuned, the "Rules" come at the end of this thread.)
5/x
I was in this camp too for quite some time! Here’s my personal history, am sure many can share something similar.
It all began with 2009 @nytimes column by their then "State of the ART" tech writer @Pogue. nytimes.com/2009/02/12/tec…
6/x
It all began with 2009 @nytimes column by their then "State of the ART" tech writer @Pogue. nytimes.com/2009/02/12/tec…
6/x
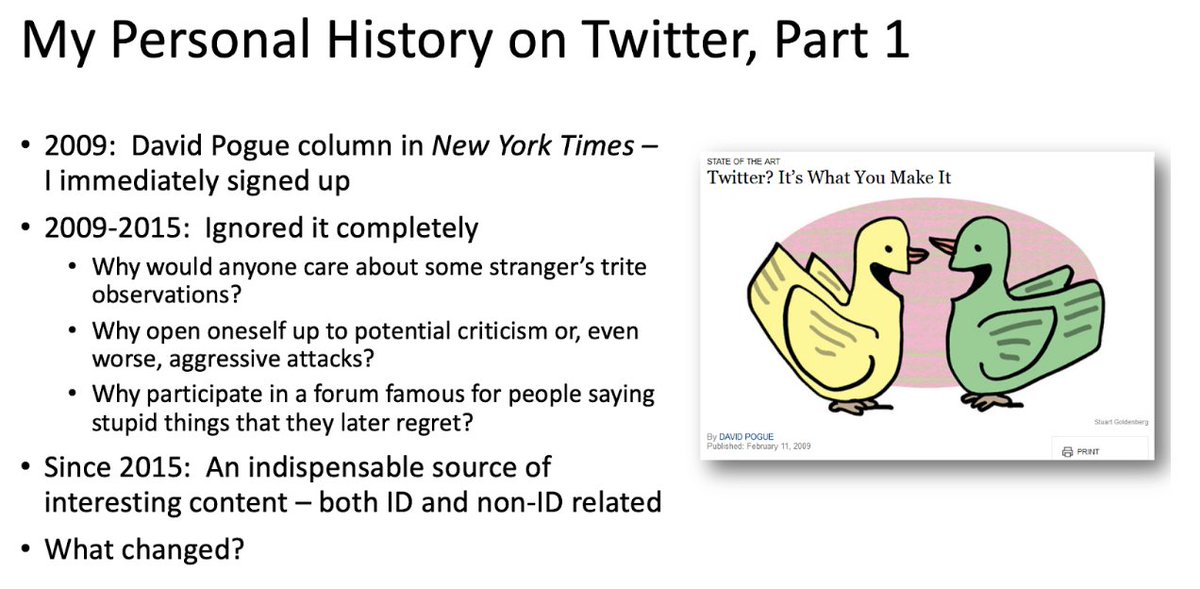
Here’s what changed -- three things in particular.
7/x
7/x

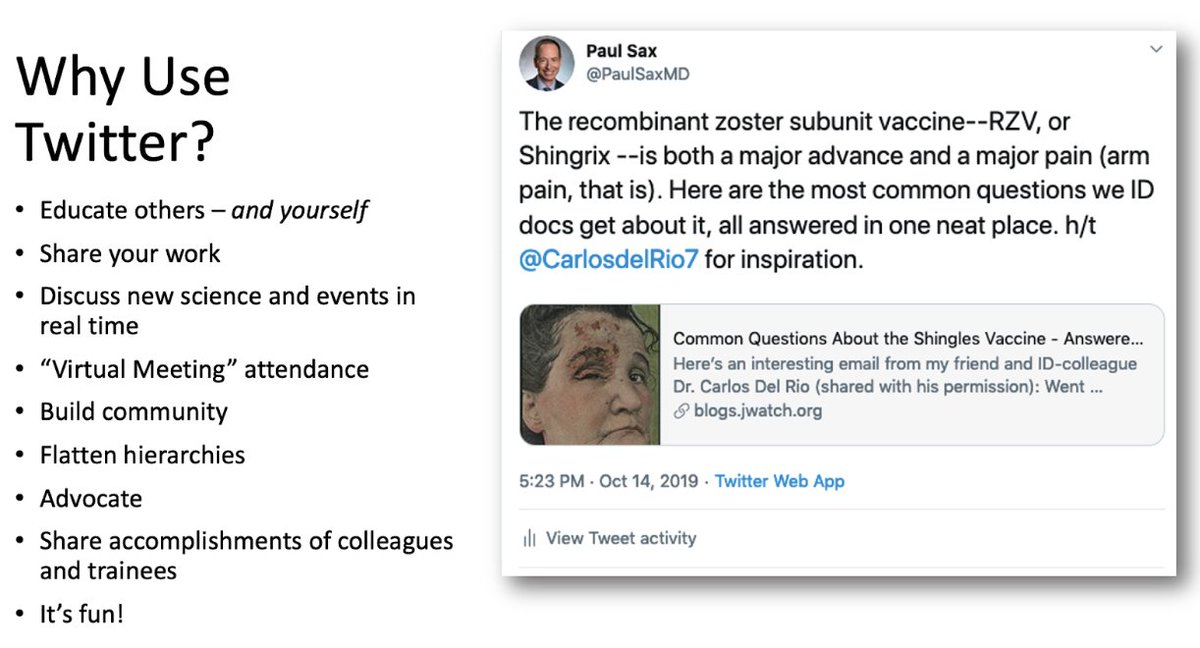
So why use Twitter? Am sure there are other reasons, but here are mine.
8/x
8/x
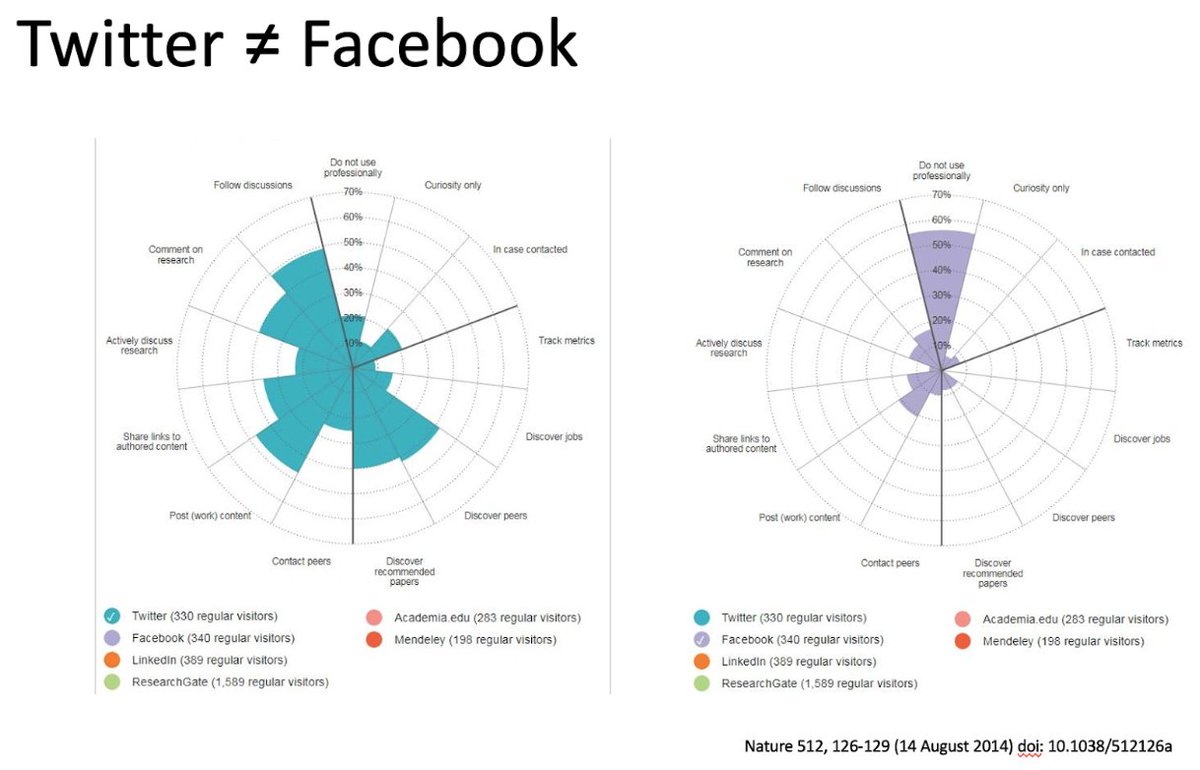
Those on other social media platforms (notably FB and instagram) might wonder how this differs.
Note that people are vastly more likely to use Twitter for professional reasons. (I got this slide from either @CarlosdelRio7 or @GermHunterMD, thank you for sharing!)
9/x
Note that people are vastly more likely to use Twitter for professional reasons. (I got this slide from either @CarlosdelRio7 or @GermHunterMD, thank you for sharing!)
9/x
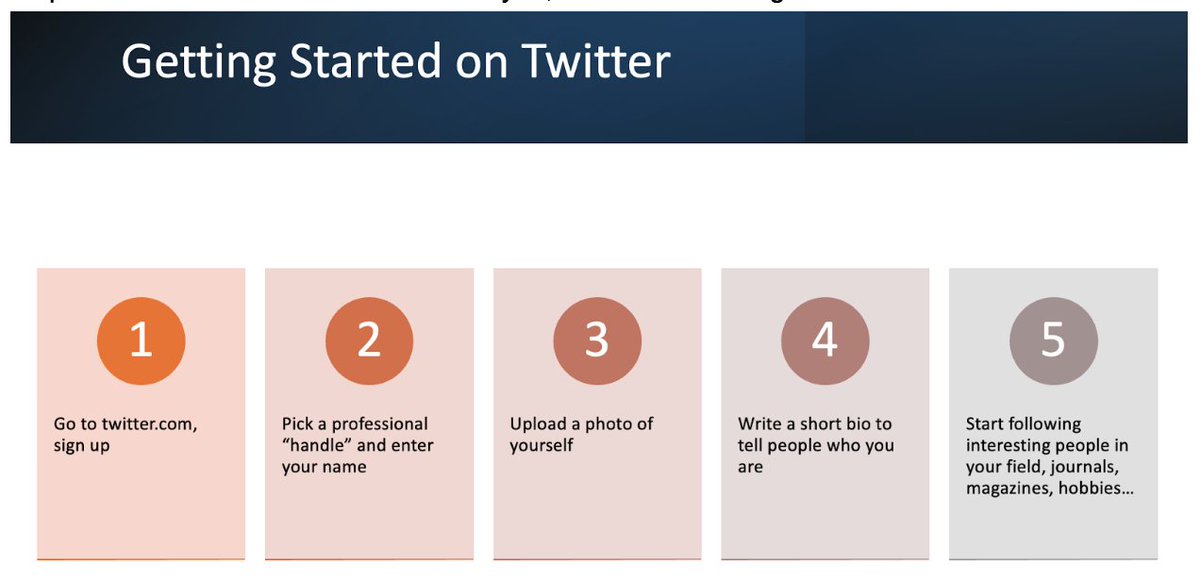
If you're reading this for the first time, and don't have an account, here’s how to get started.
10/x
10/x
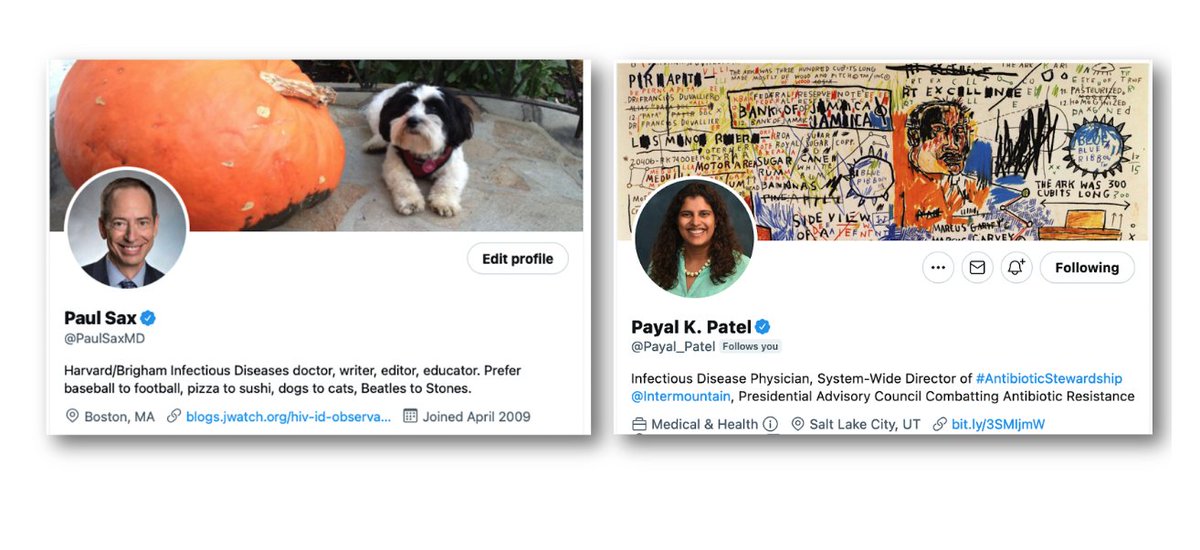
My profile, plus one of my co-presenter’s at this IDWeek session.
11/x
11/x
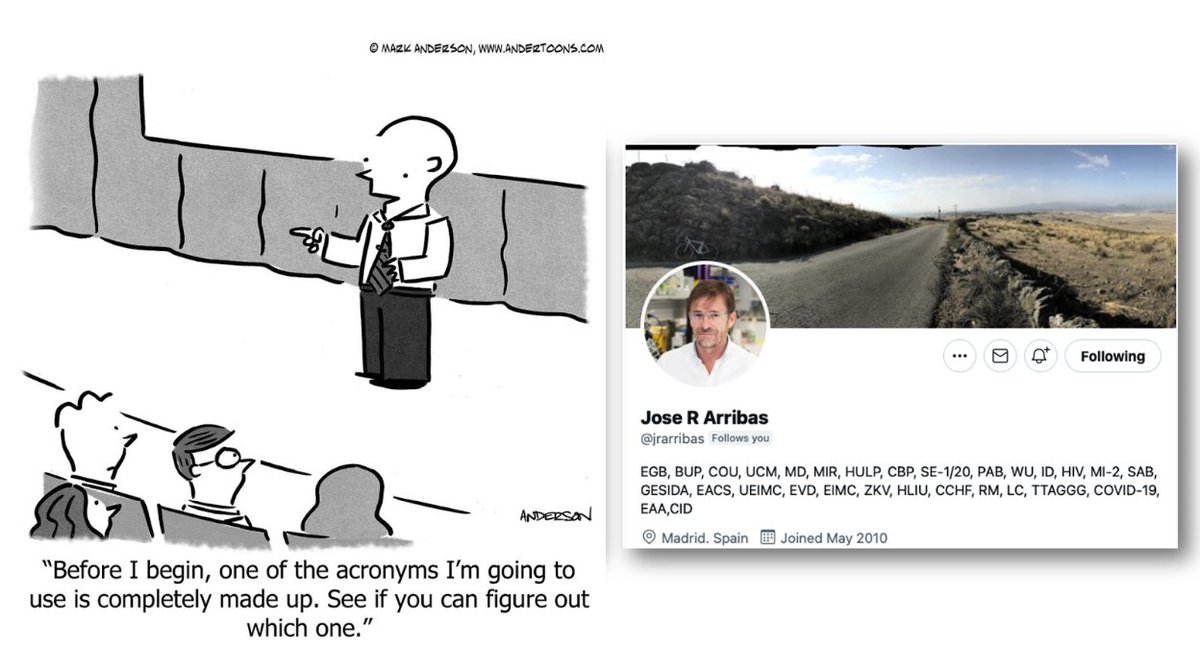
Can't resist sharing @jrarribas' profile, which makes me laugh every time I see it! 😂
(By the way, he assures me all the acronyms are real. Es verdad!)
12/x
(By the way, he assures me all the acronyms are real. Es verdad!)
12/x
Certainly you might still have questions or concerns. I address some of them here.
Note I prefer not to have the app on my phone (too distracting), but ymmv.
... and #5, by the way, is a joke.
14/x
Note I prefer not to have the app on my phone (too distracting), but ymmv.
... and #5, by the way, is a joke.
14/x

Read or publish something of interest, and want to share it?
Here's a paper published in @CIDJournal by @DrJRMarcelin et al with an important equity message.
15/x
Here's a paper published in @CIDJournal by @DrJRMarcelin et al with an important equity message.
15/x

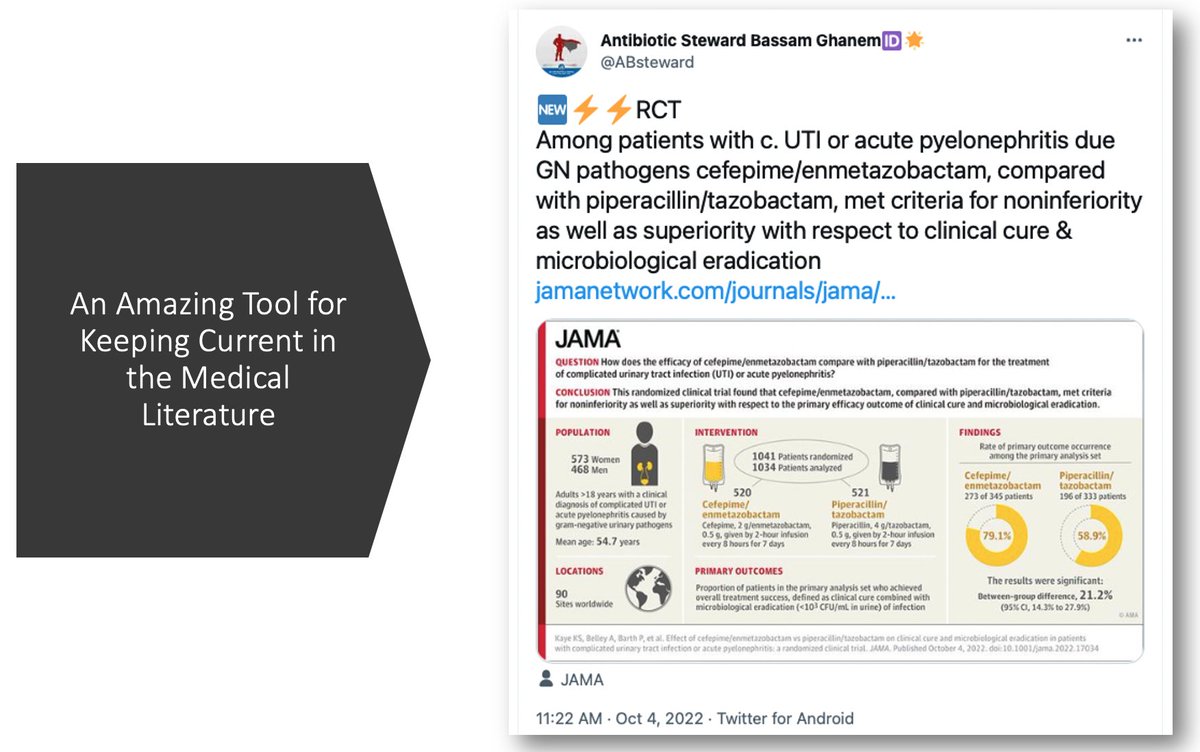
Keeping up with the literature is greatly facilitated by this site, especially with smart and prolific posters such as @ABsteward.
FYI, had never even *heard* of cefepime/enmetazobactam before this post. Hey -- you can learn a lot here!
16/x
FYI, had never even *heard* of cefepime/enmetazobactam before this post. Hey -- you can learn a lot here!
16/x
Sometimes authors of important studies start a dialogue with readers, answering their queries.
So much better (and faster) than traditional “Letters to the Editor” in journals, which can take weeks or even months to come out.
17/x
So much better (and faster) than traditional “Letters to the Editor” in journals, which can take weeks or even months to come out.
17/x

One of the most useful teaching strategies is to put together an educational Twitter thread of linked posts, or “tweetorial” -- and @tony_breu is a master.
Even the @NEJM agrees!
18/x
Even the @NEJM agrees!
18/x

Here’s a recent ID-related gem, which delves into that pesky 100,000 number for "true" UTI.
Where did that come from?
19/x
Where did that come from?
https://twitter.com/tony_breu/status/1487891320345702414?s=20&t=_yZ3qSMgnyfLs8l-Y91X3A
19/x

@GermHunterMD posted this extraordinary thread that both educates and muses -- at least if you're an ID geek like us.
BTW, if you’re about to take your ID boards and have limited time, read this thread!
20/x
BTW, if you’re about to take your ID boards and have limited time, read this thread!
https://twitter.com/GermHunterMD/status/1315102412634423298?s=20&t=KxSWvMOrGtmpWGHteOQ_oA
20/x

For me, keeping up with the latest science on Covid19 would not have been possible without smart and generous scientists sharing their expertise, such as @DrJLi and @EricTopol, among *many* others.
The field simply moves too fast.
The field simply moves too fast.

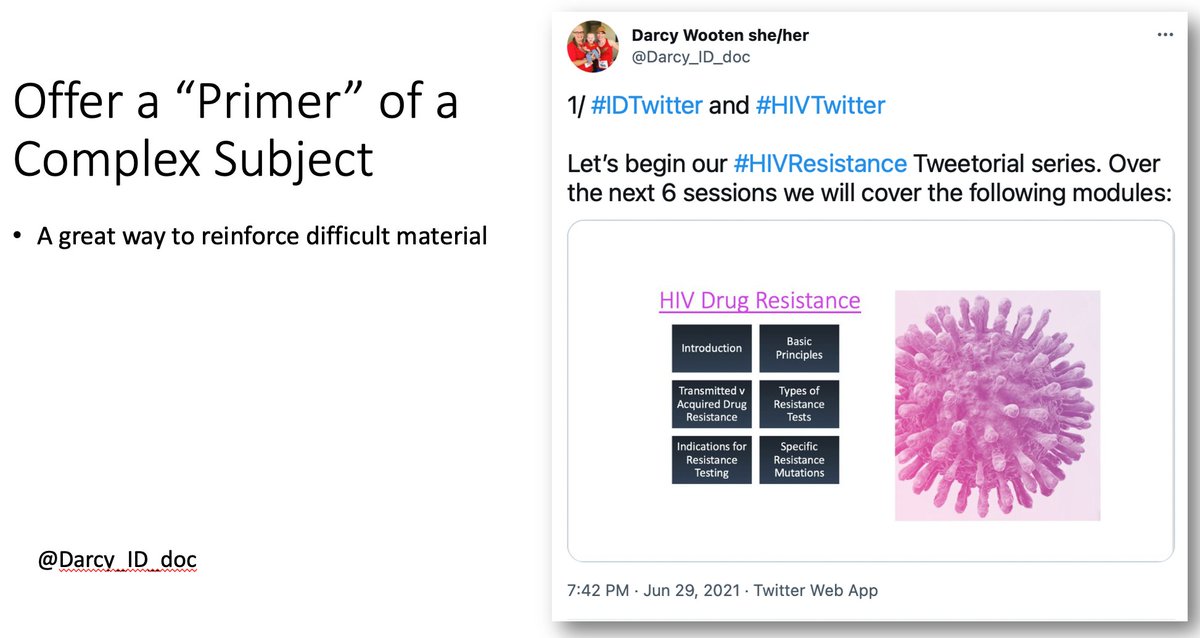
So if you've figured out a good way to teach a complex subject, sharing it via a Tweetorial is just the thing!
Here @Darcy_ID_doc offers this stellar review of HIV resistance testing.
22/x
Here @Darcy_ID_doc offers this stellar review of HIV resistance testing.
https://twitter.com/Darcy_ID_doc/status/1410020966684446726?s=20&t=5_hKRcT-kB-zJDeZiYgZBA
22/x
A brief digression to make sure we’re in compliance with accreditation guidelines ... 🐶
23/x
23/x

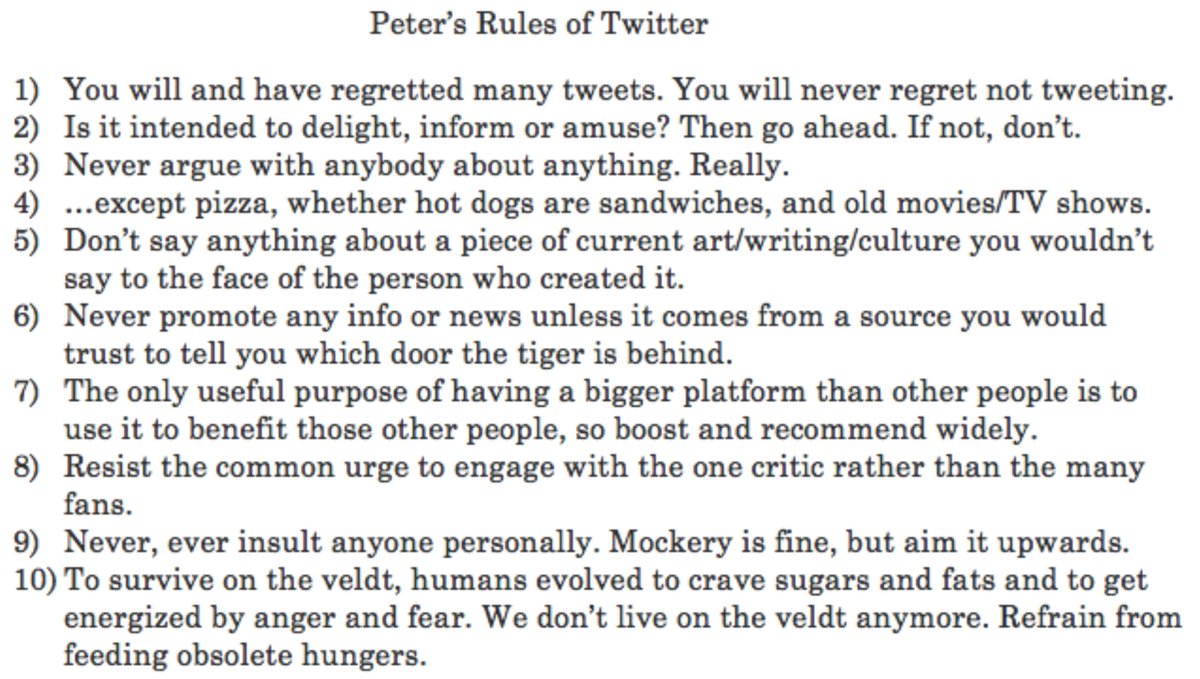
Now, how to stay out of trouble -- because that's a real problem here, and one best avoided.
For that, I turn repeatedly to @waitwait's very funny host @petersagal, and his Rules of Twitter. True wisdom -- for here and for life!
24/x
For that, I turn repeatedly to @waitwait's very funny host @petersagal, and his Rules of Twitter. True wisdom -- for here and for life!
https://twitter.com/petersagal/status/1457742811638472713?s=20&t=IbvY7RvcFn_ITmsBOlyrrA
24/x
Wrapping up with some take-homes, mostly focusing on the positives -- which on balance still outweigh the negatives, at least for me.
As @Pogue wrote way back in 2009, "DON’T KNOCK IT TILL YOU’VE TRIED IT!"
25/x
As @Pogue wrote way back in 2009, "DON’T KNOCK IT TILL YOU’VE TRIED IT!"
25/x

• • •
Missing some Tweet in this thread? You can try to
force a refresh














