The iGel is a great supraglottic airway device
But like other supraglottic airway devices (SAD) it's not foolproof
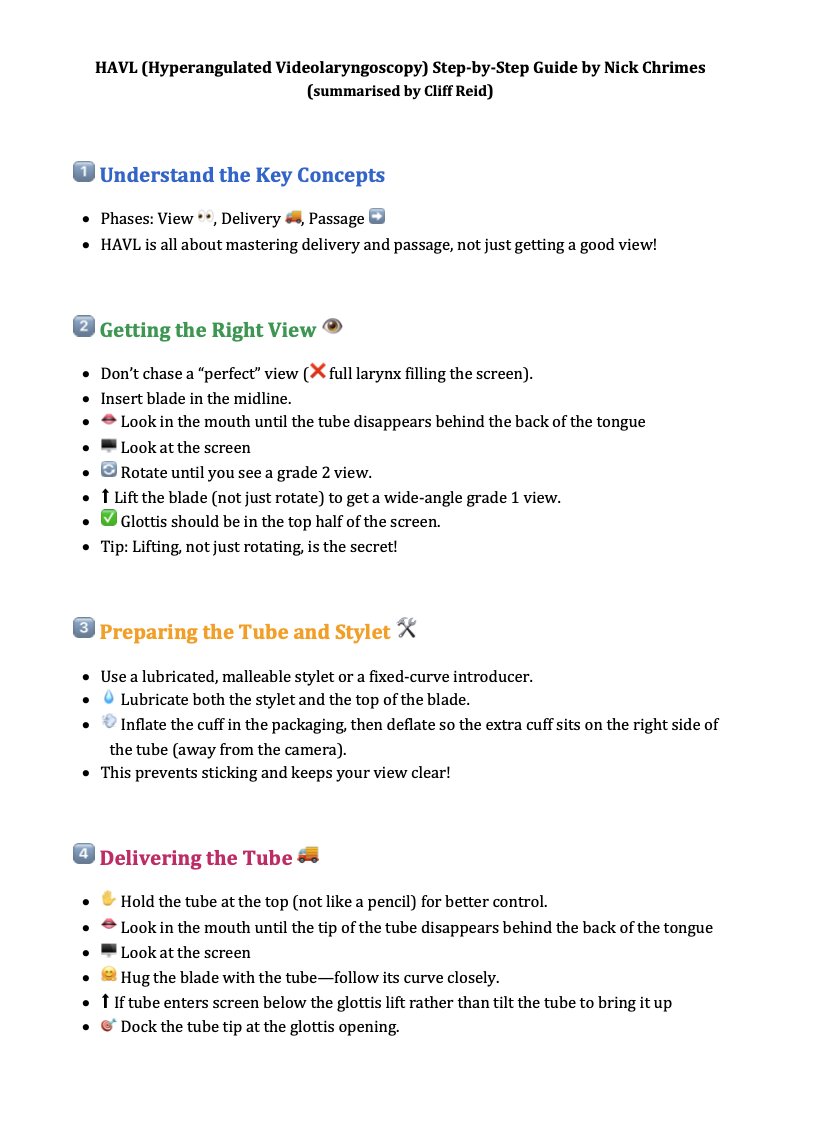
Here's how to maximise your success with the iGel - a thread 🧵
But like other supraglottic airway devices (SAD) it's not foolproof
Here's how to maximise your success with the iGel - a thread 🧵
Adequately positioned SADs produce a good seal and no leak 

Ideally the iGel cuff should sit snugly over the larynx




The tip will be in the proximal oesophagus which also allows for the passage of a gastric tube through a dedicated lumen in the device

For the right fit it needs to be:
1. Right size
2. Inserted correctly
1. Right size
2. Inserted correctly
1. Right size
The manufacturer recommends a weight based formula
size 3 for weight < 50 kg
size 4 for weight 50–90 kg
size 5 for weight > 90 kg
The manufacturer recommends a weight based formula
size 3 for weight < 50 kg
size 4 for weight 50–90 kg
size 5 for weight > 90 kg

However absolute body weight does not reliably predict airway size
When people eat more and put on weight they don't necessarily put on more airway
When people eat more and put on weight they don't necessarily put on more airway

An alternative sex based formula has been proposed - size 4 for women and size 5 for men
In a comparative study of weight-based vs sex-based insertion size selection in 900 patients, sex-based was significantly more successful
pubmed.ncbi.nlm.nih.gov/30336273/
In a comparative study of weight-based vs sex-based insertion size selection in 900 patients, sex-based was significantly more successful
pubmed.ncbi.nlm.nih.gov/30336273/

Now we've selected size we're onto point 2: Inserting Correctly
To get to the right seating position over the larynx the iGel has to get round the tongue
Otherwise insertion can potentially catch the tongue carrying it posteriorly & even folding it, preventing proper placement
To get to the right seating position over the larynx the iGel has to get round the tongue
Otherwise insertion can potentially catch the tongue carrying it posteriorly & even folding it, preventing proper placement
One way to clear the tongue for a single operator is rotation
Eg. inserting it into the mouth in the 'normal' orientation, rotating it 90° while inserting further then rotating 90° in the other direction to seat it
Or inserting it 'upside down' & rotating 180° on insertion
Eg. inserting it into the mouth in the 'normal' orientation, rotating it 90° while inserting further then rotating 90° in the other direction to seat it
Or inserting it 'upside down' & rotating 180° on insertion
Studies of these methods suggest there may be some advantage using a rotation technique - faster insertion, higher success rate, higher leak pressure, and less blood staining
pubmed.ncbi.nlm.nih.gov/24773470/
journals.lww.com/ijaweb/Fulltex…
pubmed.ncbi.nlm.nih.gov/24773470/
journals.lww.com/ijaweb/Fulltex…
Alternatively, getting round the tongue can be achieved by moving the tongue forward, by means of a chin lift / jaw thrust
This can be achieved by a single operator, sometimes with the thumb in the mouth, although this isn't recommended in non-muscle relaxed patients
This can be achieved by a single operator, sometimes with the thumb in the mouth, although this isn't recommended in non-muscle relaxed patients

The simplest & easiest way to achieve tongue clearance is to have an assistant provide the airway opening manoeuvres while the operator inserts the iGel
'2 person technique' is recommended for optimal facemask ventilation, & is appropriate for optimal supraglottic insertion too
'2 person technique' is recommended for optimal facemask ventilation, & is appropriate for optimal supraglottic insertion too

My suggested 4 step sequence for simple iGel insertion for non-expert providers (which in my view would include most non-anaesthetists) would be as follows
1. Optimise patient position
Ear-to-sternal notch horizontal alignment with neck flexion never lets you down. Also called 'flextension' this is identical to the optimal direct laryngoscopy position
Ear-to-sternal notch horizontal alignment with neck flexion never lets you down. Also called 'flextension' this is identical to the optimal direct laryngoscopy position

2. Assistant opens mouth while iGel is inserted into oral cavity

3. Assistant thrusts jaw (thumbs on maxilla) while iGel is fully inserted

4. Waveform capnography is applied and gentle bagging via the iGel is started

Summary:
iGels = great but need to be sized & inserted correctly
Size F=4 M=5
Position patient -flextension
2 person insertion technique - mouth opening & then jaw thrust
Assess for ventilation, leak, & connect ETCO2
Extra Tip: easier in paralysed patient / no cricoid pressure
iGels = great but need to be sized & inserted correctly
Size F=4 M=5
Position patient -flextension
2 person insertion technique - mouth opening & then jaw thrust
Assess for ventilation, leak, & connect ETCO2
Extra Tip: easier in paralysed patient / no cricoid pressure
See here for tips on best attempt at supraglottic insertion as part of the Vortex approach
vortexapproach.org/sga
vortexapproach.org/sga
In this video one of my airway mentors @OSWinNSW covers tips on iGel insertion which I think will be of use to all us prehospital and inhospital critical care clinicians who do not get daily exposure to these devices in the operating room
Thanks for reading!
End of 🧵
End of 🧵
• • •
Missing some Tweet in this thread? You can try to
force a refresh