
The new essay on the risk-benefit assessment and ethical analysis of mandate policies at universities by Bardosh, Krug, Prasad, Høeg, et al. has been circulated among antivax groups and conspiracy publications. This essay presented multiple misleading analyses. A thread. 🧵
We can get to the cherry-picked numbers later, but the major issue is that they framed their arguments by comparing numbers that are not comparable, numbers that have different risk profiles. Apples and oranges. They did it in three charts. jme.bmj.com/content/early/…
In Figure 1a, they compared the number of COVID hospitalization prevented against the number of Serious Adverse Events (SAEs) reported in Pfizer's trial. They plotted the two numbers on the same chart when the two bars have different units and different risks, as annotated here. 

Not only are these two numbers not a proper pair for risk and benefit analysis since the SAEs involved are transient, mostly non-hospitalized events while the hospitalized COVID have long-term consequences; they conveniently ignored that the Control arm of the Pfizer trial also…
…reported 398.4/million in the placebo group, making the 593.5/million value a gross overestimation. A more reasonable comparison would be COVID infections prevented (hospitalized or not) vs. SAEs. They knew the issue, they still used it.

Using the same reference and calculation, the number of infections prevented is 1e6/(81/0.28)=3,457 cases. Even ignoring their neglect of the control arm number, the risk and benefit conclusion is the opposite of theirs. 3,457 cases prevented (benefit) vs 593.5 SAE cases (harm).
Figure 1b is more egregious. They plotted the same hospitalization prevention number against grade≥3 Reactogenicity. "Reactogenicity refers to a subset of reactions that occur soon after vaccination, and are a physical manifestation of the inflammatory response to vaccination."
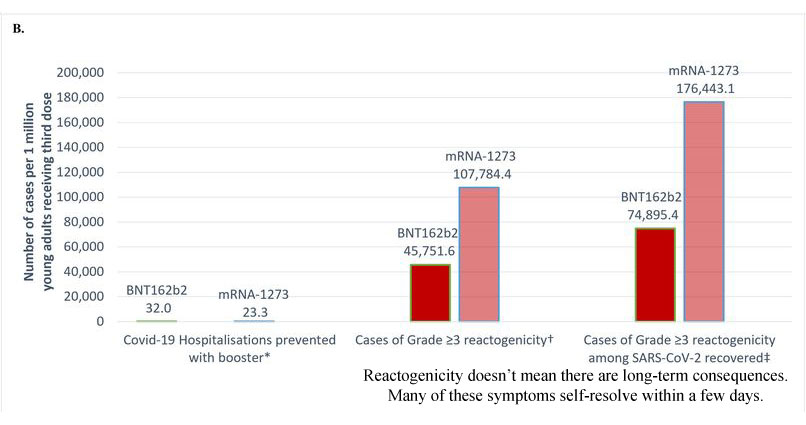
While Grade≥3 Reactogenicities (side-effects) are unpleasant and can cause some disruption to daily activity, very rarely would it require more than taking a painkiller, let alone hospitalization for which it is being compared to.
nature.com/articles/s4154…
cdc.gov/mmwr/volumes/7…
nature.com/articles/s4154…
cdc.gov/mmwr/volumes/7…
Figure 1c has the same idea but they plot against myo/pericarditis, which is the inflammation of the heart. They once again made it appear unbalanced while ignoring that these bars don't even share the same units (shouldn't be on the same chart, basic science here).
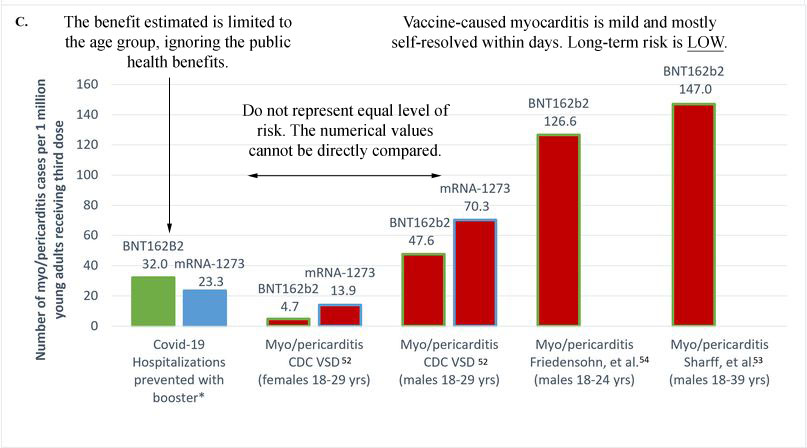
Every reference cited, and clinicians have corroborated, stated clearly that vaccination-caused myocarditis is generally mild & self-resolved, while SARSCoV2-caused ones are severe with comorbidities with other pathologies. They admitted to it themselves, and they still used it.

Besides using these misleading charts to make for a false conclusion, they also cherry-picked their numbers to minimize the benefits while maximizing the appearance of "harm".
The number of hospitalization was estimated and modified using a "needed number to vaccinate" (NNV) from the CDC for the vaccines/aOR (adjusted odds ratio) of the lowered risk for Omicron. cdc.gov/vaccines/acip/…
They picked the higher NNV from Moderna, and cherry-picked the aOR (0.28) from one Spain study, while other studies gave ranges between 0.25 up to 0.41. jamanetwork.com/journals/jama/…
We also cannot ignore the fact that their hospitalization prevented number is age-range limited while in the real world, vaccination benefits all age groups, which this essay conveniently ignored.
Given that this essay compared apples to oranges to create an appearance of a risk>benefit for this age group, it is no surprise that a study (not an essay) on risk and benefit for this came to a different conclusion. ncbi.nlm.nih.gov/pmc/articles/P…
Another Omicron-era risk & benefit study also calculated very different numbers (they compared cases prevented, plus hospitalization, which is more reasonable) and rightfully arrived at the exact opposite conclusion (note this is a PrePrint from the FDA) medrxiv.org/content/10.110…
Based on the misleading charts alone, it is clear that the essay was a conclusion looking for science-y looking justifications. However, a quick and critical look at the data and methodology expose the shortcomings fairly easily.
Some on the author list would normally not accept any evidence unless it is an RCT-backed study, justifiable or not. This is not one. This essay provides hardly any benefit to the study of COVID policies but, unfortunately, would give the antivax crowd more ammunition to harm.
An up-to-date study comparing the severity of myocarditis after vaccination vs COVID viral infection found that the postvaccination myocarditis group had a 92% lower mortality risk than the viral group.
sciencedirect.com/science/articl…
sciencedirect.com/science/articl…
• • •
Missing some Tweet in this thread? You can try to
force a refresh



