The @usda MyPlate serves as the primary educational tool for the Dietary Guidelines for Americans.
📊New CDC report: how many Americans have even heard of MyPlate? And how many tried to follow its guidance?
💣Are you ready for this?
🍽️1
📊New CDC report: how many Americans have even heard of MyPlate? And how many tried to follow its guidance?
💣Are you ready for this?
🍽️1
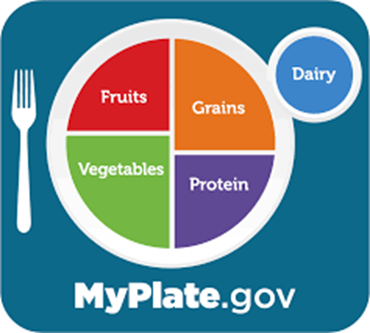

The USDA MyPlate infographic was unveiled in *2011* replacing its predecessors (pyramid, pyramid with steps) that intend to convey to Americans what defines a healthy diet. They accompany the Dietary Guidelines for Americans updated every 5 yrs.
nytimes.com/2011/06/03/bus…
🍽️2
nytimes.com/2011/06/03/bus…
🍽️2
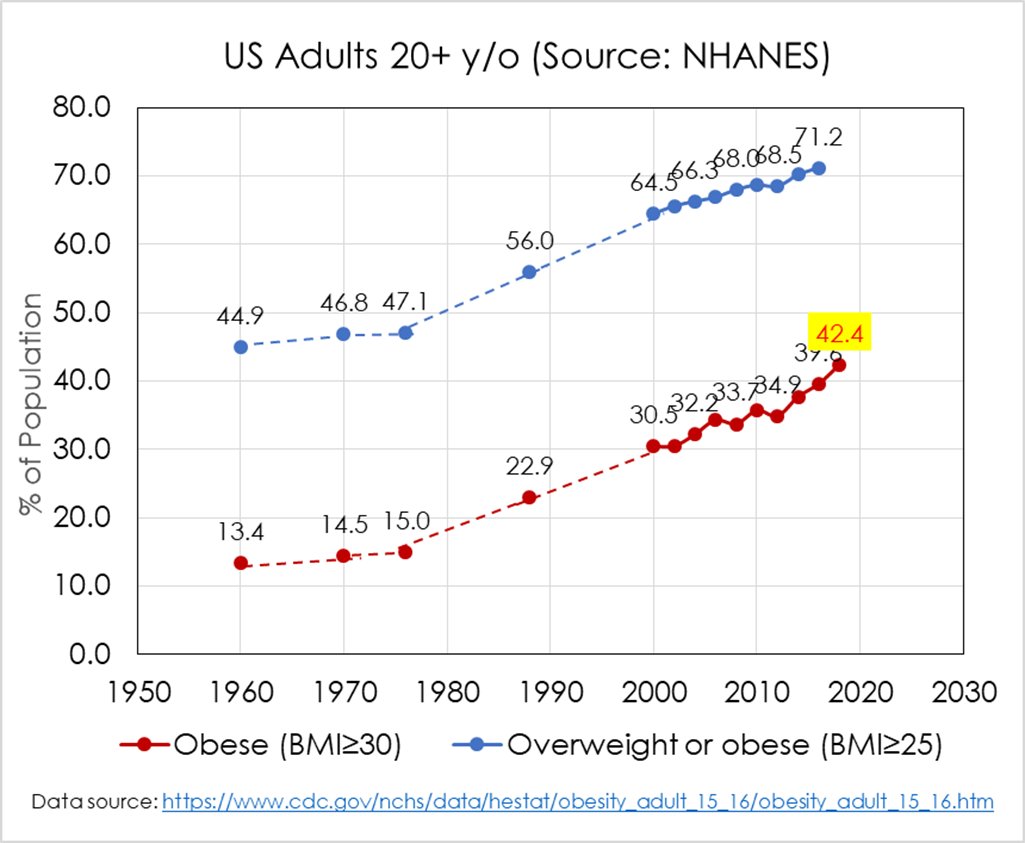
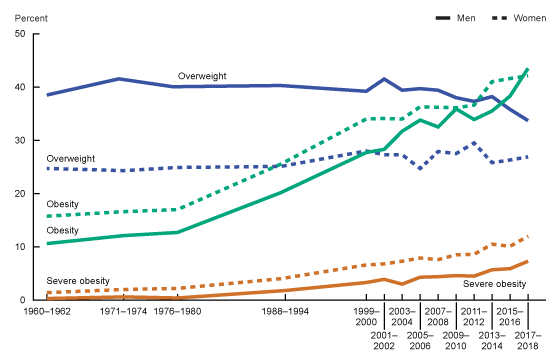
The US passively assesses the overall health of kids and adults through the @CDCgov National Health and Nutrition Examination Survey (NHANES) which conducts in-person vitals & diet/lifestyle assessments.
It's the same data that generates the trends in obesity & diet:
🍽️3
It's the same data that generates the trends in obesity & diet:
🍽️3
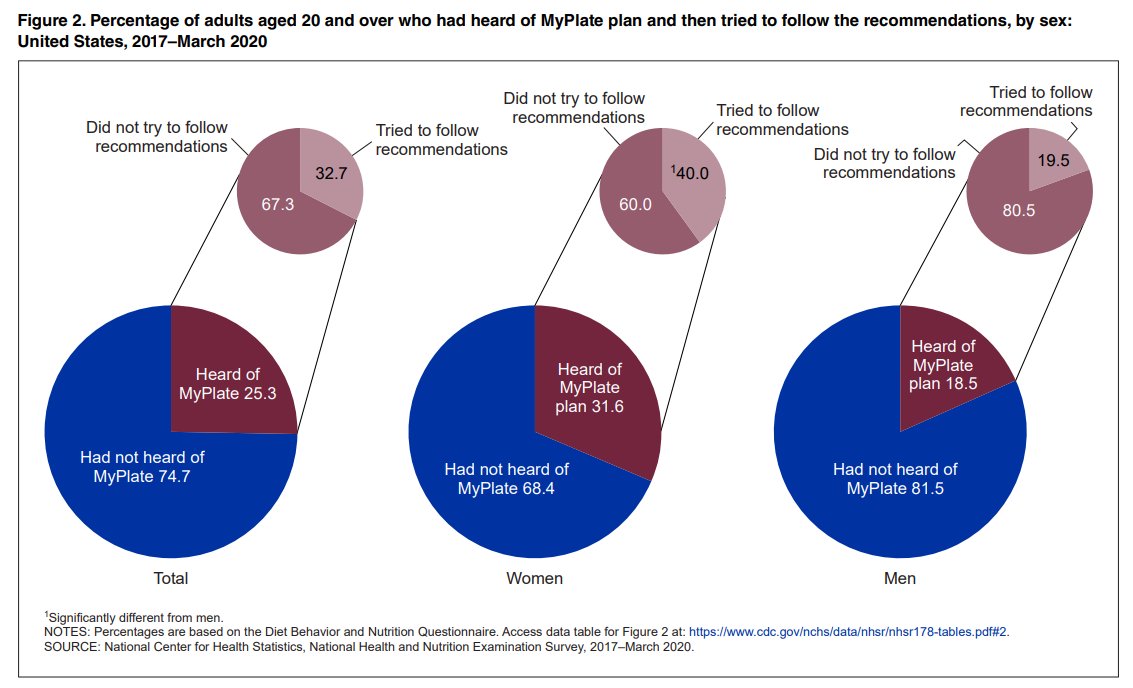
The 2017-2020 series included these questions, asking pts whether they've heard of MyPlate, and if yes, whether they've tried following its recommendations:
Have at least half of US adults ever heard of it? Maybe more?
🍽️4
Have at least half of US adults ever heard of it? Maybe more?
🍽️4

Ehhh, lower -- Sorry. A quarter. 25% of US adults have ever *heard* of MyPlate. 😬
Women were more likely than men to have heard of it.
🍽️5
Women were more likely than men to have heard of it.
🍽️5

And the big kicker -- only 8% of US adults report ever having attempted to follow its dietary guidance. LESS THAN 10% HAVE TRIED TO FOLLOW THE DIETARY GUIDELINES.
And if we're convinced pts over estimate their healthiness, then 8% is likely an OVERestimate.
🍽️6
And if we're convinced pts over estimate their healthiness, then 8% is likely an OVERestimate.
🍽️6

Ok but maybe Americans aren't familiar with "MyPlate" but are still eating consistently with its recommendations through policy etc.?
Nope. Not really.
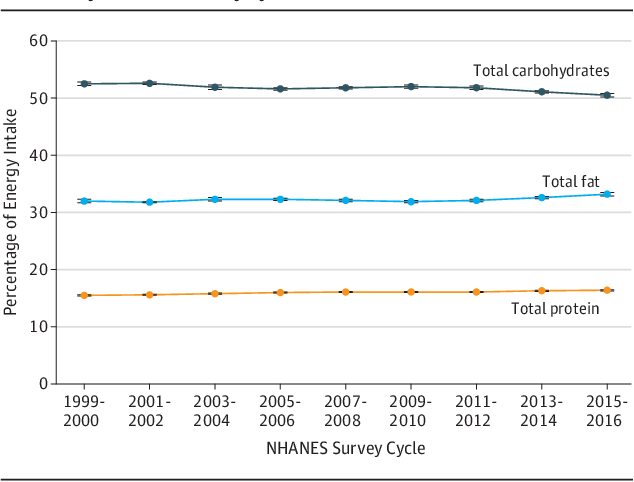
Health Eating Index (HEI) has been around for decades as a metric of guidelines adherence.
Max score is 100. Look:
🍽️7
Nope. Not really.
Health Eating Index (HEI) has been around for decades as a metric of guidelines adherence.
Max score is 100. Look:
🍽️7

Bottom line, MyPlate serves to market the guidelines but most US adults are not familiar. This leads to an overall very low <10% of adults having ever intentionally followed its diet recs. But even among those who've heard of MyPlate, only a third attempted following it.
🍽️8
🍽️8
We also know that MyPlate is just one tool of many for the dissemination and implementation of the Dietary Guidelines.
But the HEI score trends indicate not much is happening overall, regardless of the anonymity of the MyPlate.
🍽️9
But the HEI score trends indicate not much is happening overall, regardless of the anonymity of the MyPlate.
🍽️9
Here are some readings if you're interested in exploring the massive heterogeneity underlying the national averages. There are many more stories in here...
pubmed.ncbi.nlm.nih.gov/36235830/
ncbi.nlm.nih.gov/pmc/articles/P…
pubmed.ncbi.nlm.nih.gov/16256761/
pubmed.ncbi.nlm.nih.gov/27881390/
🍽️10
pubmed.ncbi.nlm.nih.gov/36235830/
ncbi.nlm.nih.gov/pmc/articles/P…
pubmed.ncbi.nlm.nih.gov/16256761/
pubmed.ncbi.nlm.nih.gov/27881390/
🍽️10
• • •
Missing some Tweet in this thread? You can try to
force a refresh