When I took on leadership of the #CHIP clinic @DanaFarber @DanaFarberNews, I was #bookedandbusy lots of #CHIP & #CCUS had been diagnosed since we rolled out our clinical NGS panel in 2014/15. But the uncertainty (the “indeterminate potential”) was disquieting.
Imagine someone hands you a grenade & says: don’t worry most don't explode. But some do. But most explosions don't kill you. But some do. We don’t know which grenade you have. Oh, and you must hold it forever
That's a hematologists diagnosing CHIP/CCUS, precursors to #MDS & #AML
That's a hematologists diagnosing CHIP/CCUS, precursors to #MDS & #AML
In truth, we're not totally compass-less. @jaiswalmdphd noted the association between high RDW & progression to myeloid neoplasm (MN) in early work.
Luca Malcovati & others noted risk was genotype specific: splicing factor mutations are higher risk than DNMT3A mutations
Luca Malcovati & others noted risk was genotype specific: splicing factor mutations are higher risk than DNMT3A mutations
But there are so many questions! Mutations in TP53 & PPM1D seem like they should be "high risk" in terms of development of MN: They show up in t-MNs, penetrance for TP53 CH --> AML was high in work by @DrPinkalDesai, and outcomes for TP53-mut MDS/AML are poor.
Evolution ofTP53 mut CH is driven by chemo exposure (per @KellyLBolton & @PapaemmanuilLab)
But what w/o chemo?
Less clonal complexity is better, sure.
But how do we put it all together?
Is 4 mutations w/ VAF <5% better or worse than 2 w/ VAF <5% if 1 of them is SRSF2?
But what w/o chemo?
Less clonal complexity is better, sure.
But how do we put it all together?
Is 4 mutations w/ VAF <5% better or worse than 2 w/ VAF <5% if 1 of them is SRSF2?
Today @ #ASH22, it was an honor to introduce the Clonal Hematopoiesis Risk Score (CHRS), as a first step towards integrated clinical risk stratification for CHIP and CCUS!
ash.confex.com/ash/2022/webpr…
ash.confex.com/ash/2022/webpr…
We used individuals with sequenced exomes from the UK Biobank to derive our model. There were a total of 193,743 people examined and 11,337 of them had either CHIP or CCUS 

We definitively confirmed genotype specificity for MN risk and defined high risk CHIP/CCUS genotypes as those with mutations in: splicing factor genes, AML-like genes (IDH1/2, RUNX1, FLT3), and JAK2.
Single DNMT3A mutant CHIP/CCUS was the sole "low risk" genotype.
Single DNMT3A mutant CHIP/CCUS was the sole "low risk" genotype.
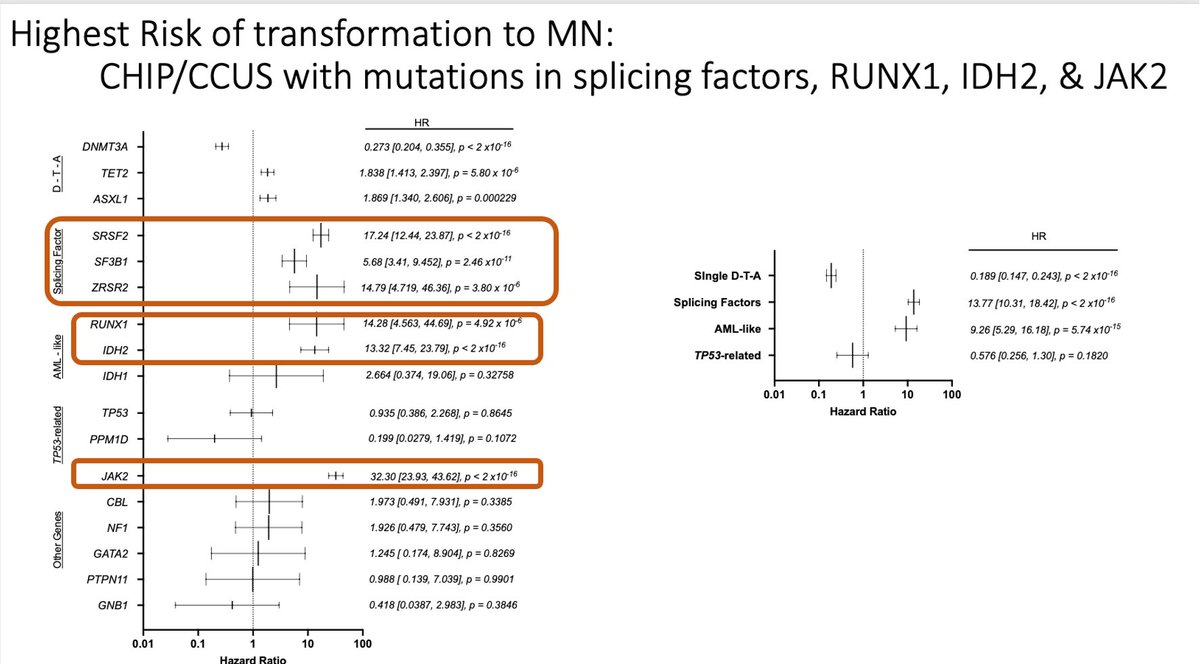

No associations was apparent for MN and TP53 or PPM1D. But, as we were prioritizing identifying a low risk population with minimal risk of MN (particularly of the deadly variety), we empirically included TP53 as a "high risk" genes with negligible effect on our final model.

we used demographics, lab values, and molecular features in conditional probability-based recursive partitioning analysis. This allowed us to identify 8 features most important for classifying MN into risk groups and the range of MN probabilities was 0.7% to 85%!

Multivariable Cox regression 1) confirmed statistical importance of each feature & 2) derived statistical weights informing on the relative contribution of each feature to individual risk. Prognostic features and their CHRS values are as in the table below:
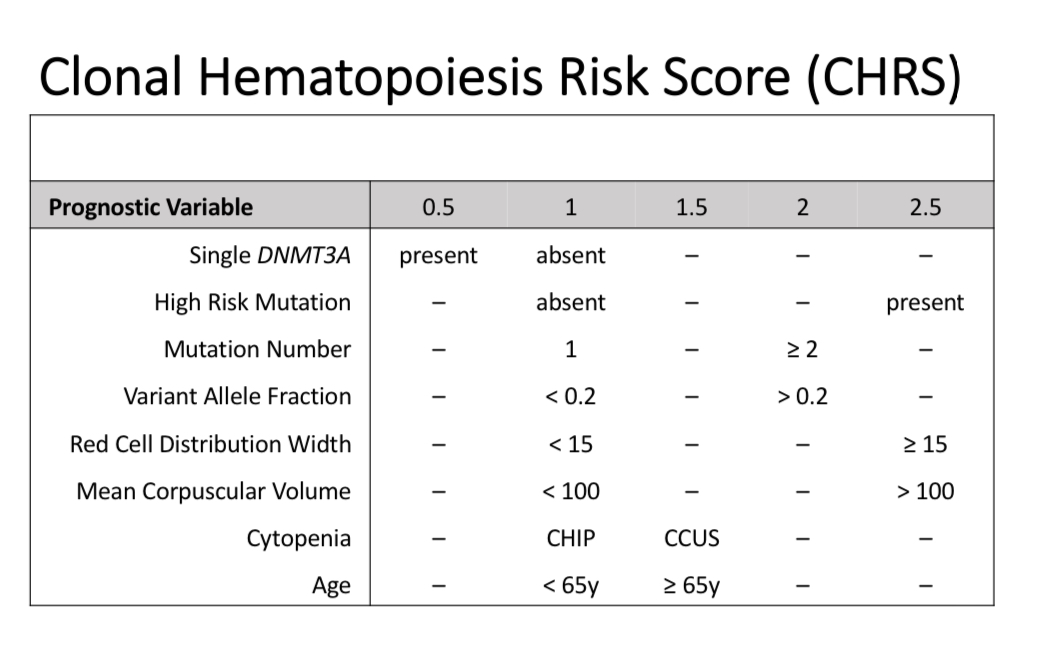
CHRS values ranged from 7.5 - 15.5.
Low risk = CHRS values ≤ 9.5
Intermediate risk = CHRS 10 - 12
High risk = CHRS values ≥ 12.5
Discriminating capability of our model was great, indicated by c-index of ~0.8 in derivation (n=11337) & validation (n = 16274) cohorts.
Low risk = CHRS values ≤ 9.5
Intermediate risk = CHRS 10 - 12
High risk = CHRS values ≥ 12.5
Discriminating capability of our model was great, indicated by c-index of ~0.8 in derivation (n=11337) & validation (n = 16274) cohorts.

Hematology patients have a higher pretest probability of incidence MN relative to a population cohort of healthy volunteers w/ incidentally discovered CH. So we externally validated our model in independent clinical cohorts from University of Pavia and @DanaFarber/@BrighamHeme
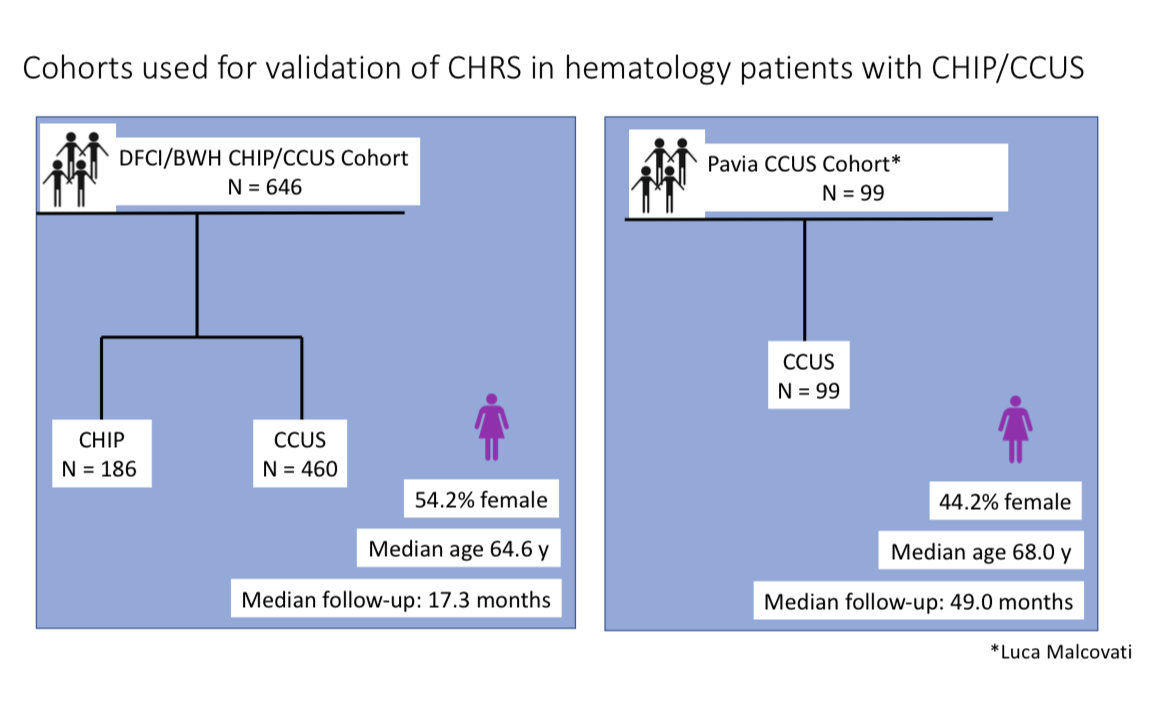
Despite short follow-up times, most progression events were in people characterized as high risk by CHRS and the c-index for both patient cohorts was > 0.7, validating the CHRS in typical clinical settings!

I'm most excited about how the CHRS can help us communicate the complexity of MN risk to patients CHIP/CCUS. And utility in helping us define high risk populations most suitable for clinical trials.
In addition to prospective validation, future work will address 3 issues:
In addition to prospective validation, future work will address 3 issues:
1- In derivation & validation cohorts, mCA ⬆️ risk of incident MN. Counting myeloid mCA as "high risk" lesions improves the CHRS c-index. We don't routinely obtain SNP arrays for CCUS. This finding + prior work by @abhinrl, Steven McCarrol, & @PapaemmanuilLab suggests we should!
2- Large cohorts with serial samples will help us understand how the CHRS values change over time (clonal dynamics) & how chemo, radiation & other selection pressures impact risk determinations.
Lastly,
3- We saw that the CHRS correlated well with survival. And while in the high risk group, most of this mortality is likely MN related, MN does not explain mortality in low and intermediate risk - could the CHRS (or a variation) predict other CH-related outcomes?
3- We saw that the CHRS correlated well with survival. And while in the high risk group, most of this mortality is likely MN related, MN does not explain mortality in low and intermediate risk - could the CHRS (or a variation) predict other CH-related outcomes?

The CHRS is imperfect & will be refined as we acquire more data - much like the IPSS for MDS. Still, risk stratification in CHIP/CCUS is foundational to building early detection & primary prevention programs for MN that can have public health relevance.
Manuscript forthcoming!
Manuscript forthcoming!
This work is the result of selfless mentorship from Ben Ebert; Research volunteers who contributed data; patients who articulated their raw emotions about uncertainty, risk & regret; career development $$$ from @HAMFDP @ASH_hematology and @RWJF;
& friendly collaborators with the audacity to believe (if only just a smidge) in futures where the improbable (AML prevention) is possible!
Thx to @abhinrl, @pnatarajanmd, @AlexBickMDPhD, @c_j_gibson, @ColemanLindsley, @LuskinMarlise, Donna Neuberg, Luca Malcovati & many others!
Thx to @abhinrl, @pnatarajanmd, @AlexBickMDPhD, @c_j_gibson, @ColemanLindsley, @LuskinMarlise, Donna Neuberg, Luca Malcovati & many others!
PDF of my #ASH22 slides available for download at the link below. Always cite your sources, friends 😊
drlachelledawn.com/chrsslides
drlachelledawn.com/chrsslides
• • •
Missing some Tweet in this thread? You can try to
force a refresh