
For 2nd yr students: Lets talk Gram's stain. Firstly in pic : Plenty of pus cells seen, Gram positive cocci in chains suggestive of Streptococcus species. This is the ideal way to interpret your Gram stain when examiner asks (Start with commenting on pus cells first and then 1/n 
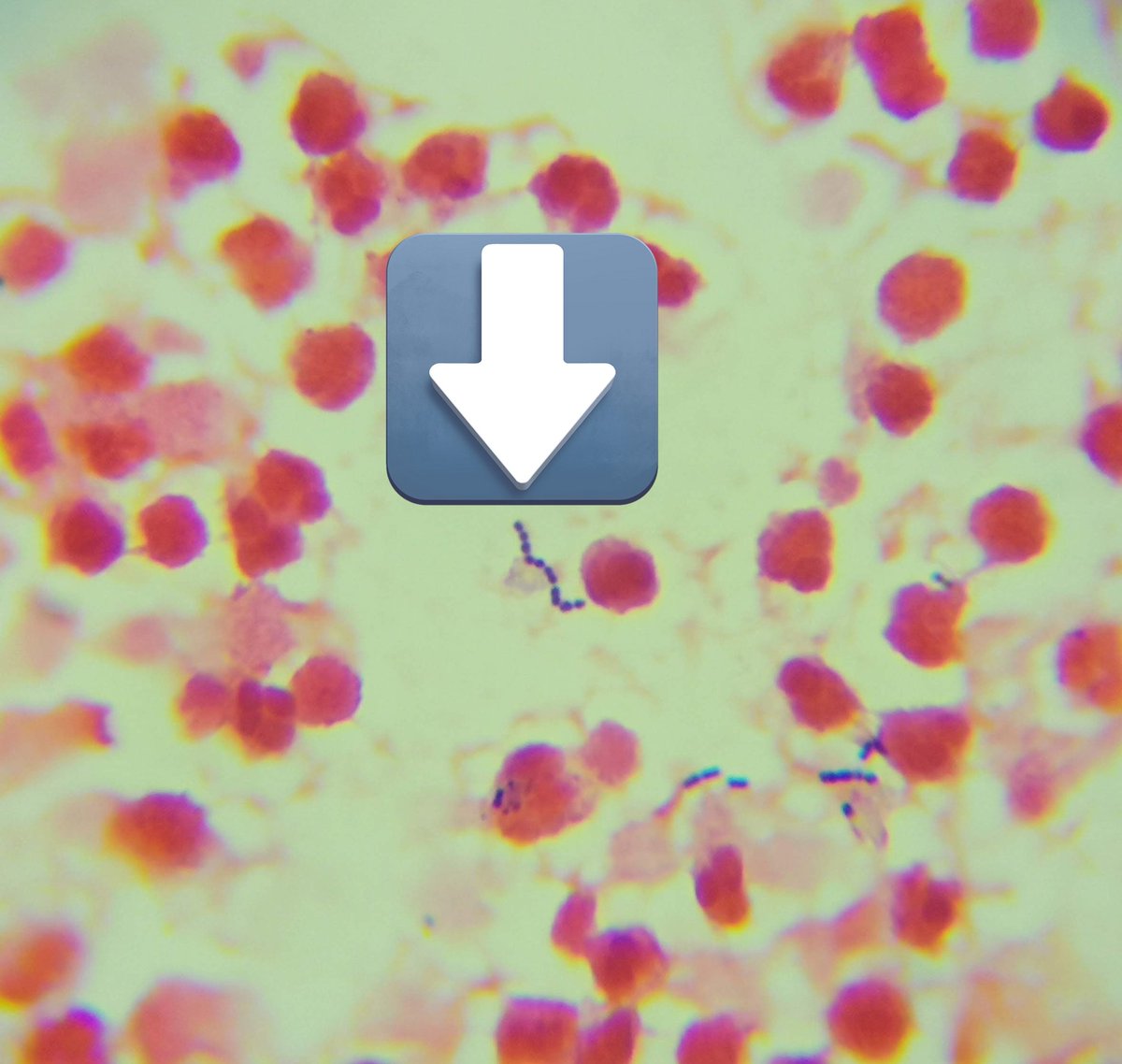
The organism, so examiner knows you know that seeing pus cells and not merely organism has its significance(indicates inflammation).Never mention d exact species, most students write GPC clusters suggestive of Staphylococcus 'aureus', you cant decide that on Microscopy alone 2/n
Principle of Gram staining:Gram Positive organisms retain primary stain better dan Gram neg organisms. Bas, dats it. Dont start peptidoglycan layer, lipopolysaccharide etc those are the theories of Gram staining, principles is only the one stated above. Then examiner will ask 3/n
Theory of Gram stain then all the points about cell wall, cytoplasm etc.
Applications of Gram stain
a)Empirical Rx
b) Appropriateness of specimen (like sputum vs saliva: more epithelial cells its saliva not useful sample in LRTI, more pus cells ✅️)
c) Spot diagnosis like 4/n
Applications of Gram stain
a)Empirical Rx
b) Appropriateness of specimen (like sputum vs saliva: more epithelial cells its saliva not useful sample in LRTI, more pus cells ✅️)
c) Spot diagnosis like 4/n
Gas gangrene i.e Absent or very few pus cells (its gangrene so no blood so no pus cells), polymicrobial and Gram Pos bacilli Box cart appearance (s/o Clostridium perfringes)
d)Selection of media (like McConkey if GNB are seen etc)
Any other questions u were asked, shoot here 5/n
d)Selection of media (like McConkey if GNB are seen etc)
Any other questions u were asked, shoot here 5/n
Next I ll post a series of Gram stain pics, you will be amazed at how much information you can get with this test which costs less than 15Rs and gives results in 15 mins or so.
Hopefully it also changes ur opinion about importance of Microbiology 6/n
Hopefully it also changes ur opinion about importance of Microbiology 6/n
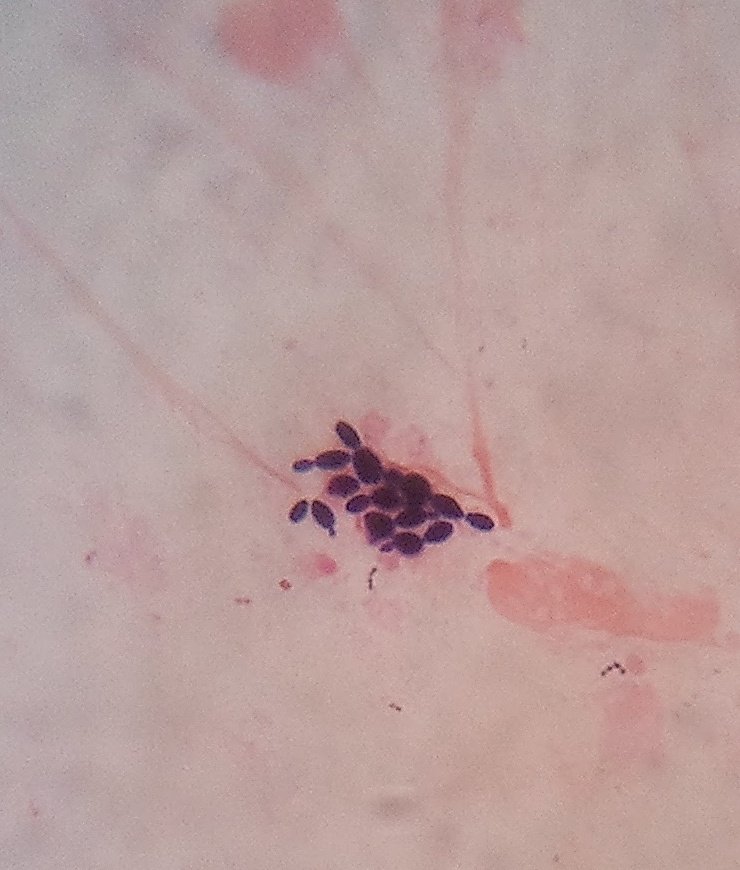
Plenty pus cells, budding yeast cells with pseudohyphae

Budding yeast cells
All the pink structures are Gram neg bacilli, Those safety pin like are Gram positive bacilli with spores which is unstained

Lanceolate shaped Gram positive diplococci with an appreciable halo (capsule), U guessed it right suggestive of Streptococcus pneumoniae (can be confirmed only by culture)

Pus cells and plenty of Gram neg diplococci(not clear in pic) in a urethral discharge. Of course N.gonorrhea (culture confirmatory)

Pus cells, branched Gram positive filamentous bacteria - Nocardia or Actinomyces species. Do modified AFB - Nocardia will be acid fast

Gram positive cocci in long chains - Suggestive of Streptococcus species. End of thread!

• • •
Missing some Tweet in this thread? You can try to
force a refresh




