NEW: @UKHSA Variant Technical Briefing 49
🔘 XBB.1.5 and CH.1.1 designated variants
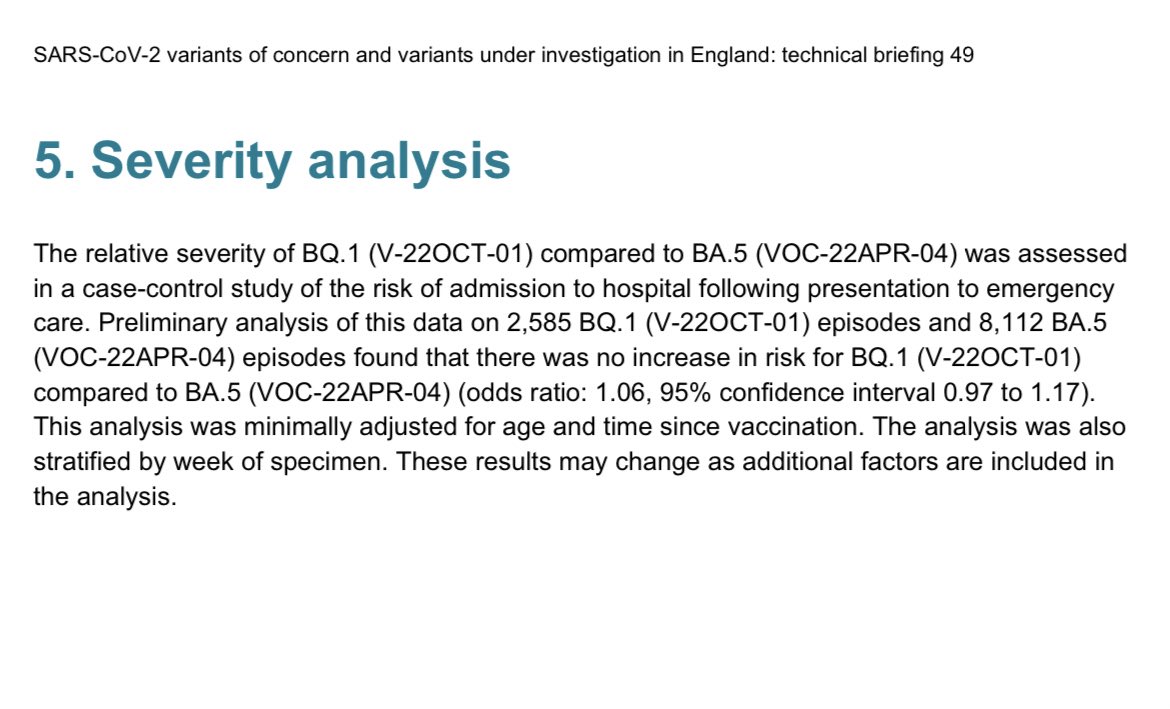
🔘 BQ.1 severity and VE estimates
assets.publishing.service.gov.uk/government/upl…
🔘 XBB.1.5 and CH.1.1 designated variants
🔘 BQ.1 severity and VE estimates
assets.publishing.service.gov.uk/government/upl…

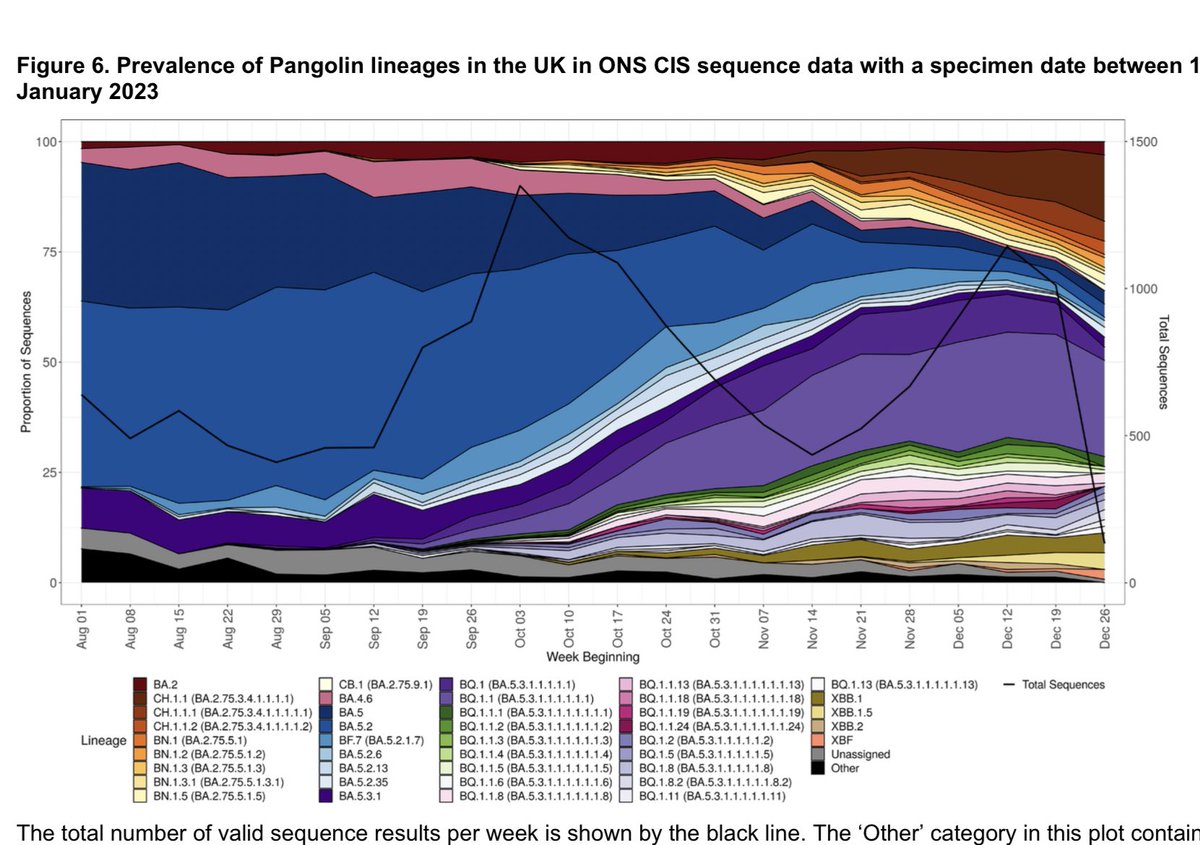
Start with overall variant picture for England to 1 Jan:
This is Omicron soup. 🍜 Each colour a different Omicron lineage.
BQ.1.1 in light purple 🟣 is the most common at 51% of cases
CH.1.1 in yellow 🟡 is 20% and growing
XBB.1.5 in dark red 🔴 is 4.5% and growing
This is Omicron soup. 🍜 Each colour a different Omicron lineage.
BQ.1.1 in light purple 🟣 is the most common at 51% of cases
CH.1.1 in yellow 🟡 is 20% and growing
XBB.1.5 in dark red 🔴 is 4.5% and growing

🛑 sampling bias warning❗️
English sequenced cases are *highly* skewed to older ages, due to prioritising samples for sequencing from hospital patients and care homes.
The median age of English 🏴 sequenced COVID-19 cases is
76 years old 👴🏻 👵🏻
English sequenced cases are *highly* skewed to older ages, due to prioritising samples for sequencing from hospital patients and care homes.
The median age of English 🏴 sequenced COVID-19 cases is
76 years old 👴🏻 👵🏻

So where possible, it is more informative to restrict analysis to community cases from ONS survey.
Smaller numbers but a closer reflection of the population.
When we do, we do see a similar pattern. Reassuring — no variant appears to be driving infection in elderly.
Smaller numbers but a closer reflection of the population.
When we do, we do see a similar pattern. Reassuring — no variant appears to be driving infection in elderly.
Now to the new variant designations CH.1.1 and XBB.1.5
There’s a lot of interest in XBB.1.1 already, so I’ll focus on CH.1.1 first.
CH.1.1 has been growing steadily in UK since early Nov.
Origin country unknown, but UK reports more CH.1.1 than any other country.
There’s a lot of interest in XBB.1.1 already, so I’ll focus on CH.1.1 first.
CH.1.1 has been growing steadily in UK since early Nov.
Origin country unknown, but UK reports more CH.1.1 than any other country.

About half of CH.1:1 sequences are from 🇬🇧 but it is reported in >60 countries globally incl New Zealand, Denmark, USA and Austria, Australia, Japan
Its a BA.2.75 sub-lineage with a bunch of antigenic mutations which make it immune evasive
@LongDesertTrain details more ⤵️
Its a BA.2.75 sub-lineage with a bunch of antigenic mutations which make it immune evasive
@LongDesertTrain details more ⤵️
https://twitter.com/longdeserttrain/status/1596199893357379584

Why is CH.1.1 interesting?
Because I’m England 🏴 it’s currently in head-to-head competition with XBB.1.5 in UK.
Although it has had a head start, it’s still spreading quickly and seemingly unhindered by XBB.1.5
Because I’m England 🏴 it’s currently in head-to-head competition with XBB.1.5 in UK.
Although it has had a head start, it’s still spreading quickly and seemingly unhindered by XBB.1.5


How do the immune evasion profiles compare?
This data from @yunlong_cao shows CH.1.1 and XBB.1.5 have similar neutralisation titres versus vaxxed + BA.5 breakthrough infection
This data from @yunlong_cao shows CH.1.1 and XBB.1.5 have similar neutralisation titres versus vaxxed + BA.5 breakthrough infection

But, XBB.1.5 remains a concern.
While numbers XBB.1.5 are small in this analysis (n~130)
XBB.1.5 is showing a higher growth rate than CH.1.1 (relative to BA.5) in England
While numbers XBB.1.5 are small in this analysis (n~130)
XBB.1.5 is showing a higher growth rate than CH.1.1 (relative to BA.5) in England

🛑 I’ve warned about over interpretation of early growth rates before ⤵️
UKHSA data is no exception. As I said above, we’d prefer to restrict growth rates to ONS survey data alone. But couldn’t because XBB.1.5 numbers were too small yet.
So interpret with caution…
UKHSA data is no exception. As I said above, we’d prefer to restrict growth rates to ONS survey data alone. But couldn’t because XBB.1.5 numbers were too small yet.
So interpret with caution…
https://twitter.com/kallmemeg/status/1611485034594160681
That said, evidence is accumulating to suggest that XBB.1.5 does have the edge in infectiousness
Due to the double nucleotide change at 486 increasing spike affinity to ACE2
h/t @yunlong_cao @SystemsVirology
Due to the double nucleotide change at 486 increasing spike affinity to ACE2
h/t @yunlong_cao @SystemsVirology


So my sense is that XBB.1.5 will eventually come to dominate.
Meanwhile, it is plausible that CH.1.1 and XBB.1.5 will grow in tandem and cooperate to increase COVID incidence in England 🏴 over the next few weeks. The size of wave is unclear, but unlikely to be BA.1/BA.2 levels.
Meanwhile, it is plausible that CH.1.1 and XBB.1.5 will grow in tandem and cooperate to increase COVID incidence in England 🏴 over the next few weeks. The size of wave is unclear, but unlikely to be BA.1/BA.2 levels.
In terms of severity of XBB.1.5, we have some early reassuring data from @PeacockFlu lab at @imperialcollege
XBB (parent lineage) acts like previous Omicron lineages with the altered entry pathway and preference for nasal 👃 cell tissue over lung 🫁
XBB (parent lineage) acts like previous Omicron lineages with the altered entry pathway and preference for nasal 👃 cell tissue over lung 🫁

We will keep a very close eye on the mutations XBB picks up, especially on spike.
As @PeacockFlu notes, #F486P may act as evolutionary credit, covering the cost of new mutations, even if detrimental, but over time such rapid evolution can result in some nasty new variants…
As @PeacockFlu notes, #F486P may act as evolutionary credit, covering the cost of new mutations, even if detrimental, but over time such rapid evolution can result in some nasty new variants…

FINALLY:
🔺New BQ.1 vaccine & severity analysis
• Risk of Hospitalisation with BQ.1 (after A&E attendance): aOR 1.06 (0.97-1.17) vs BA.5
• Vaccine effectiveness vs hospitalisation:
BQ.1 —>50% (35-62%)
BA.5 —>64% (53-72%)
BQ.1 lower but overlapping CIs.
🔺New BQ.1 vaccine & severity analysis
• Risk of Hospitalisation with BQ.1 (after A&E attendance): aOR 1.06 (0.97-1.17) vs BA.5
• Vaccine effectiveness vs hospitalisation:
BQ.1 —>50% (35-62%)
BA.5 —>64% (53-72%)
BQ.1 lower but overlapping CIs.

Well done as ever to @meera_chand & crew
@freja_kirsebom for the VE analysis
@epb41l2 and @giulia_seghezzo for the severity analysis
And many others…!
Pre-prints coming soon on some of the early data presented here. 👍🏻
@freja_kirsebom for the VE analysis
@epb41l2 and @giulia_seghezzo for the severity analysis
And many others…!
Pre-prints coming soon on some of the early data presented here. 👍🏻
Correction - this is growth relative to BQ.1.1 (not BA.5)
https://twitter.com/kallmemeg/status/1615131086647971840
Eek correction 2: CH.1.1 is dark red chunk at top right, XBB.1.5 light yellow sliver at bottom right
I’m about to pay for that damn edit button you know 😑
I’m about to pay for that damn edit button you know 😑
https://twitter.com/kallmemeg/status/1615126484095475712
• • •
Missing some Tweet in this thread? You can try to
force a refresh