ECPR for OHCA: Pre-hospital or in-hospital?
Happy to share this Editorial written with @Alice_hutin and @giovannilandoni commenting on a SR/MA by @nattiejpk investigating the role of pre-hospital #ECPR.
🧵👇 Learn more in the thread /17
🔗 bit.ly/3ZQQNNG #ResusTwitter
Happy to share this Editorial written with @Alice_hutin and @giovannilandoni commenting on a SR/MA by @nattiejpk investigating the role of pre-hospital #ECPR.
🧵👇 Learn more in the thread /17
🔗 bit.ly/3ZQQNNG #ResusTwitter

2/
#ECPR is the last rescue therapy when despite high-quality conventional CPR it is not possible to achieve ROSC.
In such situations, OHCA is considered refractory and E-CPR recently demonstrated to improve outcomes in selected patients.
#ResusTwitter
#ECPR is the last rescue therapy when despite high-quality conventional CPR it is not possible to achieve ROSC.
In such situations, OHCA is considered refractory and E-CPR recently demonstrated to improve outcomes in selected patients.
#ResusTwitter
https://twitter.com/tscquizzato/status/1496765510150770688
3/
@nattiejpk recently conducted a SRMA published on @JCVAonline investigating effect of preh initiation of #ECPR on low-flow and survival
Most evidence comes from Paris, first EMS applying preh ECPR since 2011 @LionelLamhaut @alice_hutin
@nattiejpk recently conducted a SRMA published on @JCVAonline investigating effect of preh initiation of #ECPR on low-flow and survival
Most evidence comes from Paris, first EMS applying preh ECPR since 2011 @LionelLamhaut @alice_hutin
https://twitter.com/LionelLamhaut/status/1611429560746123265#ResusTwitter
4/
Preh #ECPR is one of the 2 main strategies to provide ECPR for OHCA pts but it is not commonly adopted.
A “load and go” strategy where pts are rapidly transported with ongoing CPR is more widespread and was recently tested in 2 RCTs.
Preh #ECPR is one of the 2 main strategies to provide ECPR for OHCA pts but it is not commonly adopted.
A “load and go” strategy where pts are rapidly transported with ongoing CPR is more widespread and was recently tested in 2 RCTs.
https://twitter.com/tscquizzato/status/1496241433354936324#ResusTwitter
5/
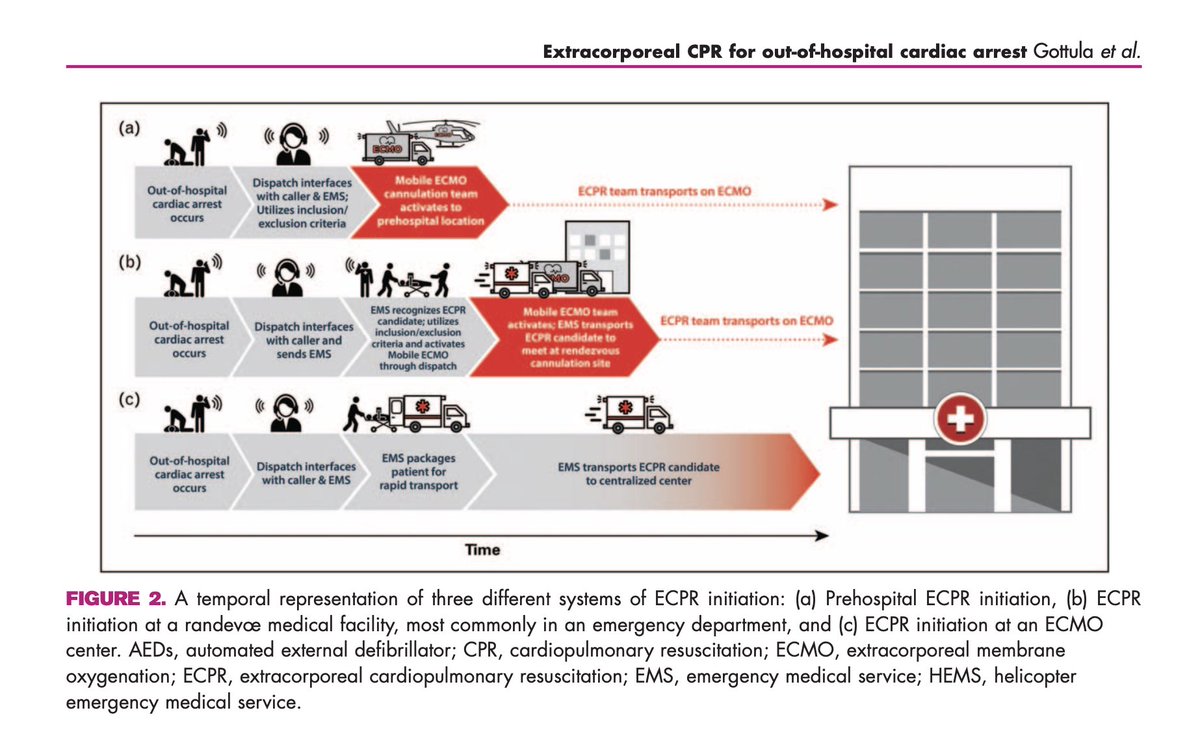
In pre-hospital #ECPR, ECMO is established at the place of OHCA (home, street) and the patient is transported once ECMO cannulation is completed.
Pre-hospital E-CPR potentially reduces low-flow by avoiding delays due to pt extraction and ambulance transport.
#ResusTwitter
In pre-hospital #ECPR, ECMO is established at the place of OHCA (home, street) and the patient is transported once ECMO cannulation is completed.
Pre-hospital E-CPR potentially reduces low-flow by avoiding delays due to pt extraction and ambulance transport.
#ResusTwitter
6/
In their meta-analysis of pre-hospital ECPR, Kruit and colleagues reported a mean low-flow time of 61 min.
Since shorter low-flow times are associated with better outcomes and pre-h ECPR pursues this goal, one might expect a shorter low-flow 🤔
sciencedirect.com/science/articl…
In their meta-analysis of pre-hospital ECPR, Kruit and colleagues reported a mean low-flow time of 61 min.
Since shorter low-flow times are associated with better outcomes and pre-h ECPR pursues this goal, one might expect a shorter low-flow 🤔
sciencedirect.com/science/articl…
7/
Mean low-flow times for in-hospital E-CPR in the ARREST trial was 59 min and in the Prague OHCA study 61 min but often very variable and much higher outside the setting of randomized trials.
#ResusTwitter
Mean low-flow times for in-hospital E-CPR in the ARREST trial was 59 min and in the Prague OHCA study 61 min but often very variable and much higher outside the setting of randomized trials.
#ResusTwitter

8/
It’s difficult staying within 60’ of low-flow (golden hour for E-CPR), even when initiating #ECPR in the pre-hospital setting.
Paris strategy significantly reduced low-flow with similar cannulation time, success and complications.
pubmed.ncbi.nlm.nih.gov/28414164/ #ResusTwitter
It’s difficult staying within 60’ of low-flow (golden hour for E-CPR), even when initiating #ECPR in the pre-hospital setting.
Paris strategy significantly reduced low-flow with similar cannulation time, success and complications.
pubmed.ncbi.nlm.nih.gov/28414164/ #ResusTwitter

9/
Concerning survival after pre-hospital #ECPR, @nattiejpk calculated a pooled survival to hospital discharge of 23%.
The absence of a comparator and the small number of studies and patients included prevent from drawing firm conclusions.
#ResusTwitter
Concerning survival after pre-hospital #ECPR, @nattiejpk calculated a pooled survival to hospital discharge of 23%.
The absence of a comparator and the small number of studies and patients included prevent from drawing firm conclusions.
#ResusTwitter

10/
Only one observational study in Paris compared pre-hospital #ECPR with in-hospital E-CPR (N=525).
Pre-hospital cannulation was an independent predictor of higher survival (OR 2.9, 95% CI 1.5–5.9) and favorable neurological outcome (OR 2.9, 95% CI 1.3–6.4).
#ResusTwitter
Only one observational study in Paris compared pre-hospital #ECPR with in-hospital E-CPR (N=525).
Pre-hospital cannulation was an independent predictor of higher survival (OR 2.9, 95% CI 1.5–5.9) and favorable neurological outcome (OR 2.9, 95% CI 1.3–6.4).
#ResusTwitter


11/
The potential reduction in low-flow that pre-hospital ECPR can offer and increase in survival are not only determined by initiating ECMO at OHCA site but also by EMS organization, rapid identification of eligible pts, and early activation of ECPR team and ECMO implementation
The potential reduction in low-flow that pre-hospital ECPR can offer and increase in survival are not only determined by initiating ECMO at OHCA site but also by EMS organization, rapid identification of eligible pts, and early activation of ECPR team and ECMO implementation
12/
It is essential to consider that preh #ECPR cannulation is performed in a more complex/unpredictable environment
In-h ECPR is in a more controlled setting with immediate availability of more equipment/diagnostics/HCPs, facilitating the procedure and complications management
It is essential to consider that preh #ECPR cannulation is performed in a more complex/unpredictable environment
In-h ECPR is in a more controlled setting with immediate availability of more equipment/diagnostics/HCPs, facilitating the procedure and complications management
13/
This is a not exhaustive list of pros and cons of pre-hospital initiation of #ECPR
Others to add?
jcvaonline.com/article/S1053-… #ResusTwitter
This is a not exhaustive list of pros and cons of pre-hospital initiation of #ECPR
Others to add?
jcvaonline.com/article/S1053-… #ResusTwitter

14/
RCTs comparing preh vs in-h #ECPR are currently lacking.
ON-SCENE trial is randomizing in The Netherlands to preh ECPR provided through HEMS vs conventional resuscitation.
We will have to wait until 2026 to see the results.
#ResusTwitter @ECMOphile
RCTs comparing preh vs in-h #ECPR are currently lacking.
ON-SCENE trial is randomizing in The Netherlands to preh ECPR provided through HEMS vs conventional resuscitation.
We will have to wait until 2026 to see the results.
#ResusTwitter @ECMOphile
https://twitter.com/ECMOphile/status/1470815350262575105?s=20&t=NHykGQEVZFvDI1PpuQ_mOQ
15/
Aiming “no-flow 0” with early CPR remains the cornerstone: bystanders have an unquestionable role and are the primary drivers of good outcome
#ECPR has little benefit without bystander CPR
Apps to alert FRs should be first implemented!
Aiming “no-flow 0” with early CPR remains the cornerstone: bystanders have an unquestionable role and are the primary drivers of good outcome
#ECPR has little benefit without bystander CPR
Apps to alert FRs should be first implemented!
https://twitter.com/tscquizzato/status/1504499327049342987@ffsemeraro
16/
It is clear that treating refractory OHCA pts with prehospital #ECPR (but also in-hospital) poses unique logistical challenges in addition to clinical ones
Preh ECPR requires considerable resources/skills not universally available in the pre-hospital setting
#ResusTwitter
It is clear that treating refractory OHCA pts with prehospital #ECPR (but also in-hospital) poses unique logistical challenges in addition to clinical ones
Preh ECPR requires considerable resources/skills not universally available in the pre-hospital setting
#ResusTwitter
17/
When #ECPR is applied, low-flow time should be minimized and preh ECPR could be the most effective way but there is very low certainty of evidence supporting it.
The best strategy remains to be demonstrated and may be dependent on system-specific factors.
#ResusTwitter
When #ECPR is applied, low-flow time should be minimized and preh ECPR could be the most effective way but there is very low certainty of evidence supporting it.
The best strategy remains to be demonstrated and may be dependent on system-specific factors.
#ResusTwitter
If you enjoyed this thread:
1️⃣ Follow me for daily tweets or threads on resuscitation and cardiac arrest: @tscquizzato
2️⃣ Jump to the top of this thread and retweet the very first tweet:
1️⃣ Follow me for daily tweets or threads on resuscitation and cardiac arrest: @tscquizzato
2️⃣ Jump to the top of this thread and retweet the very first tweet:
https://twitter.com/tscquizzato/status/1616800254497538052
• • •
Missing some Tweet in this thread? You can try to
force a refresh