
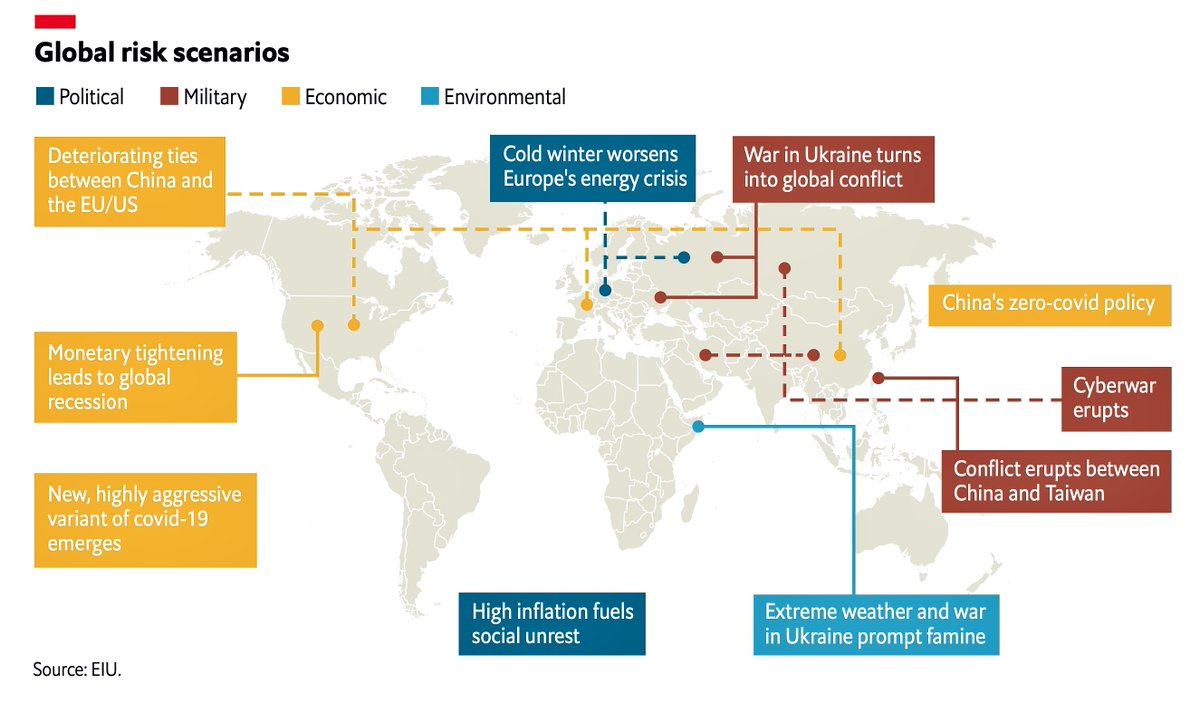
This comes from the 2023 EIU global risk assessment. The trouble is, lifting China's #zeroCOVID policy is the very thing propelling the evolution of a “new, highly aggressive variant of COVID”🧵 mkto-ab220141.com/NzUzLVJJUS00Mz… 
China is too dependent on the productivity of its factory workforce. Factories are ill-ventilated sardines cans ripe for COVID eruptions disrupting manufacturing. Mass death/injury means worker supply is less than demand, pushing up the cost of labour. axios.com/2022/12/16/the…
Mortality from pandemics has historically increased the value of labour. The plague probably helped to end serfdom in Europe. Chinese manufacturing depends on cheap labour, but with #infiniteCOVID, CCP serfdom will struggle, and this critical cogwheel in the economy will stutter.

There is a risk that the resulting economic and social unrest may crash the Chinese property market, mentioned as a risk in the EIU 2022 report. Reduced manufacturing will lessen supply and drive up inflation worldwide, forcing “fast monetary tightening”. mkto-ab220141.com/NzUzLVJJUS00Mz…

Once again, I would issue a stern warning to economists that biosecurity risks to world socioeconomic stability are being gravely underestimated. The socioeconomic impacts of COVID are only just beginning to make themselves felt. The political storm is only just brewing.
Those familiar with infectious diseases in other species will know they can be as much an existential threat to species survival as climate change from asteroid strikes. As with anthropogenic climate change, we are not taking this seriously enough.

Pestilence has forever been accompanied by famine and war. That there are signs of growing geopolitical military instability at a time of worldwide pestilence is likely no coincidence. The more we let rip with the pestilence, the greater the amplification of geopolitical risk.

• • •
Missing some Tweet in this thread? You can try to
force a refresh









