
Wherein @Samantha_Burn @timothyjlayton @borisvabson and I take on the unenviable task of defending medical paperwork:
"Rationing Medicine Through Bureaucracy: Authorization Restrictions in Medicare"
on NBER: nber.org/papers/w30878
and ungated: zarekcb.github.io/PriorAuth_Web.…
"Rationing Medicine Through Bureaucracy: Authorization Restrictions in Medicare"
on NBER: nber.org/papers/w30878
and ungated: zarekcb.github.io/PriorAuth_Web.…
Health care bureaucracy is the last truly bipartisan issue. It covers 1-4% of US GDP(!), and no matter who you ask, it's horrible and wasteful.
The dilemma is: Half of admin costs (as per Cutler below) are about managed care! Policies meant to restrain rapid cost growth.
The dilemma is: Half of admin costs (as per Cutler below) are about managed care! Policies meant to restrain rapid cost growth.
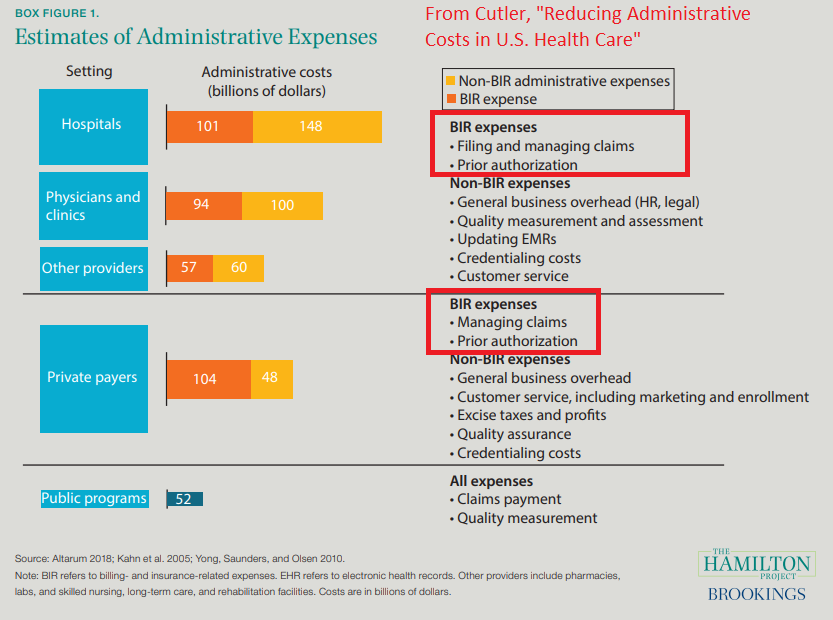
This gives us a trade-off: Either we face wasteful health care spending, or costly administration.
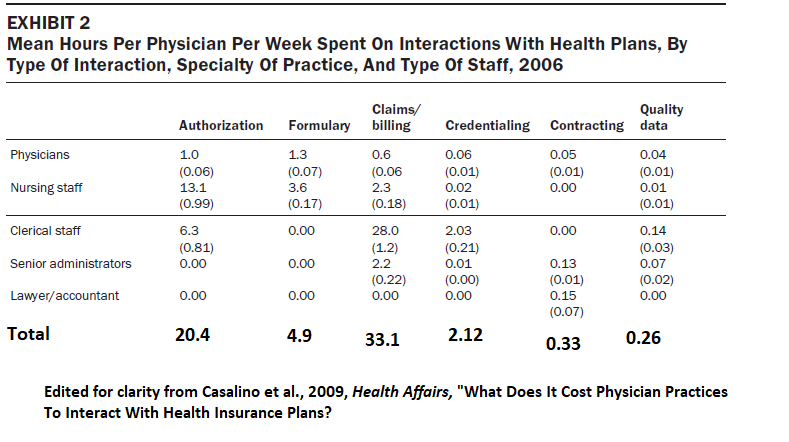
In our study, we consider this trade-off in the case of prior authorization restrictions. Prior auth is a big source of admin effort, and especially requires a lot of skilled labor
In our study, we consider this trade-off in the case of prior authorization restrictions. Prior auth is a big source of admin effort, and especially requires a lot of skilled labor
Prior auth requires that the insurer review a prescribed drug/service before granting insurance coverage. As you might imagine, this has AMA opposition, who say that prior auth leads to hospitalization and dying.*
*based on a survey of what doctors _think_ prior auth does
*based on a survey of what doctors _think_ prior auth does

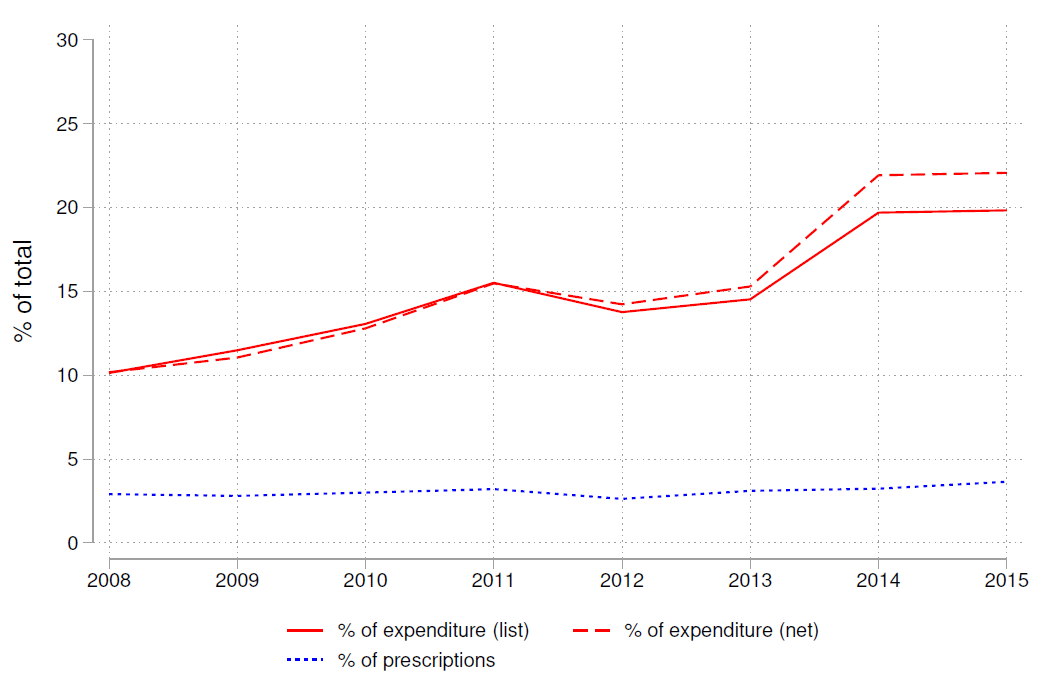
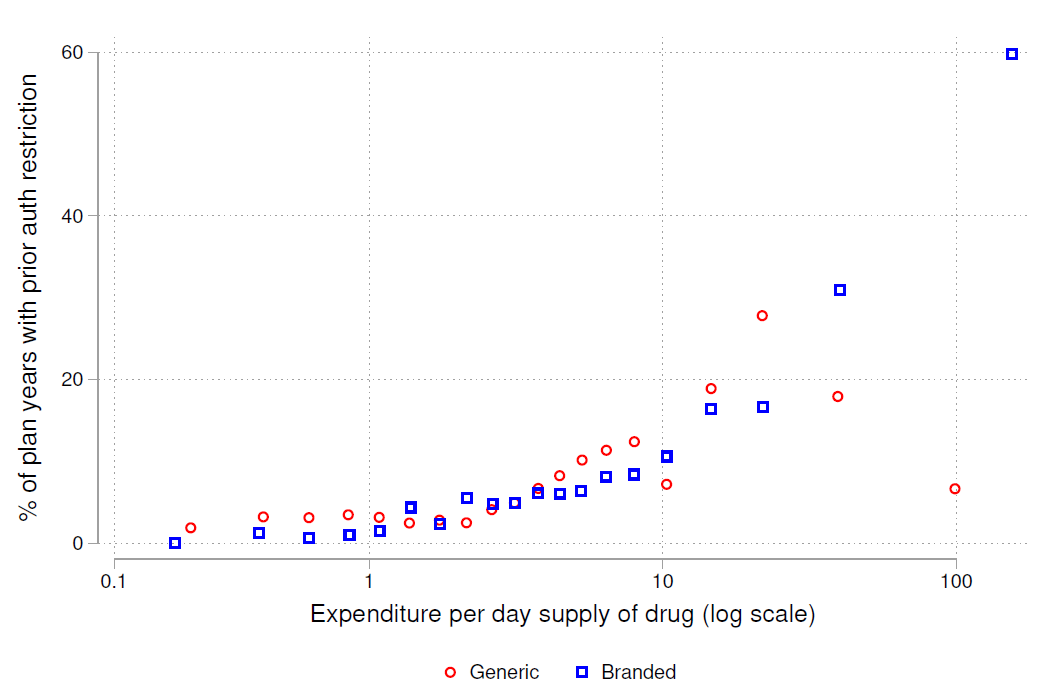
We study it in Medicare Part D drug insurance. The use of prior auth has been steadily climbing: up to 5% of filled prescriptions, but well over 20% of spending (both gross + net). That's because it generally applies to expensive, niche, on-patent drugs.
In the low-income subsidy program, beneficiaries often get randomly assigned to one of many possible default plans, each of which restricts different drugs. We compare, for a given drug, utilization for those randomly assigned to plans that restrict the drug vs. plans that don't
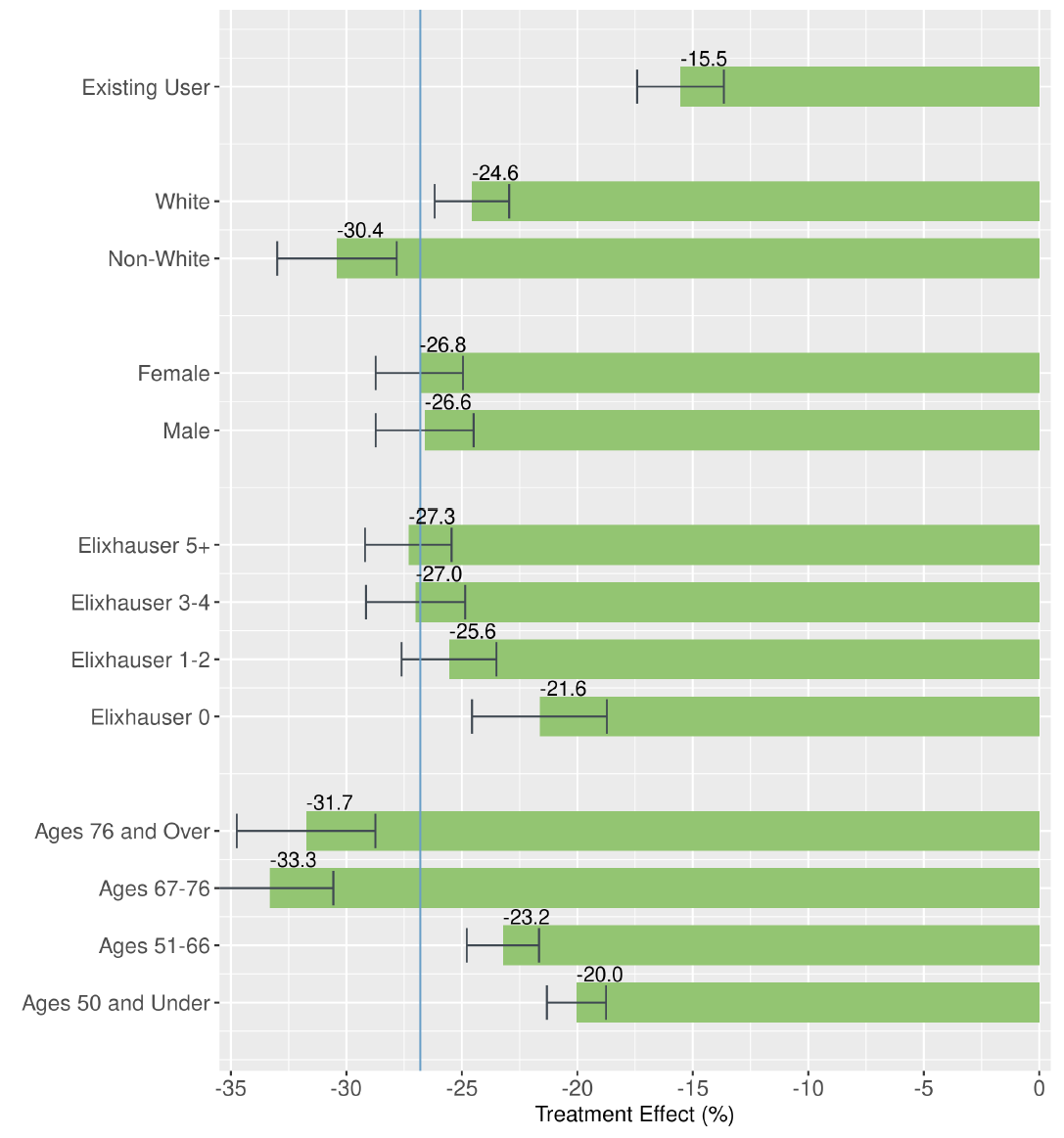
We estimate that prior auth on a drug reduces its use by 26.8%, with bigger effects for non-white and older patients.
To understand how patients substitute in response, we estimate a demand system for nearly every drug in Part D.
To understand how patients substitute in response, we estimate a demand system for nearly every drug in Part D.
We estimate that roughly half of patients substitute to a therapeutic substitute, with the other half taking no drug (or something outside the therapeutic class).
That sounds high, but in my prior work on HDHPs we found that *all* of the substitution margin was care vs. no care.
That sounds high, but in my prior work on HDHPs we found that *all* of the substitution margin was care vs. no care.
On net, prior auth reduces spending per-beneficiary-year by $96, or 3.6% (incl. reductions for restricted drugs and increases for unrestricted substitutes)
This is the benefit of prior auth, but how does it compare to the costs? Two relevant costs.
This is the benefit of prior auth, but how does it compare to the costs? Two relevant costs.
First cost: Admin hassle. We quantify it using prior estimates of the cost of doing prior auth ($11-$31 per application). We estimate admin costs of $10 per beneficiary-year, only 1/10th of the spending reductions. For some drug classes this ratio is even larger.
Second cost: Patient value. What would patients be willing to pay for the drugs they forgo?
Probably less than costs. Financial savings from prior auth are $86 per beneficiary-year, WTP is $13-$80 under a range of assumptions. Prior auth is equivalent to a ~$227/year copay.
Probably less than costs. Financial savings from prior auth are $86 per beneficiary-year, WTP is $13-$80 under a range of assumptions. Prior auth is equivalent to a ~$227/year copay.
(as an aside: willingness to pay is a crude measure of patient value, but it's all we have. In the paper, we try two approaches to quantifying effects on health, but even with a million patients, we don't have the statistical power to say much.)
Administration isn't just pure waste--it can actually reduce costs! (in this case)
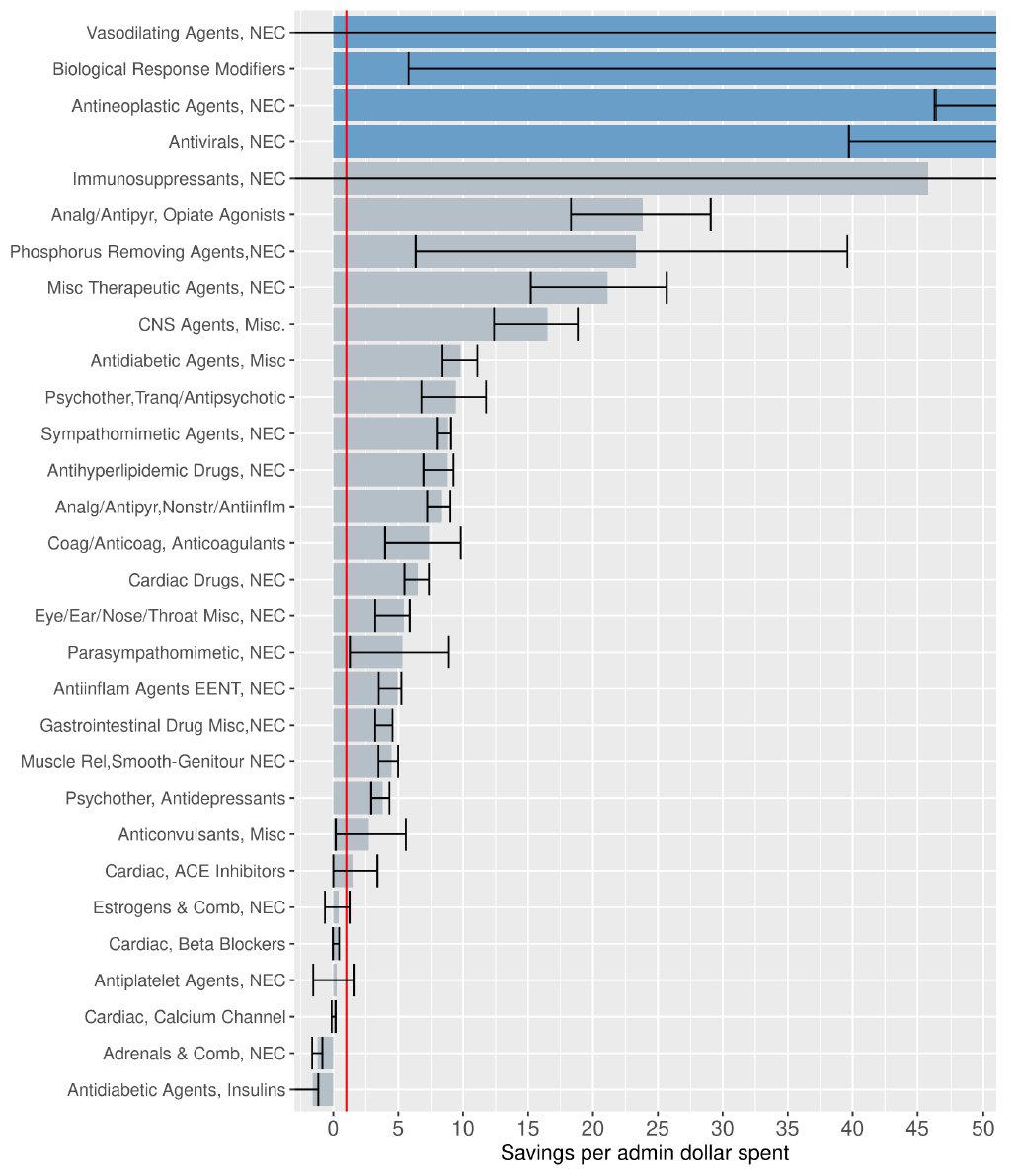
A key factor is that prior auth was targeted well. We simulated the effects of prior auth on everything else. Big decreases in spending, but even bigger admin costs. Don't prior auth statins!
A key factor is that prior auth was targeted well. We simulated the effects of prior auth on everything else. Big decreases in spending, but even bigger admin costs. Don't prior auth statins!
In health care there's been a big surge of papers showing inefficient underuse of low-cost treatments. But we can forget that we also have inefficient *overuse* of high-cost treatments, incl. expensive drugs but also things like C-sections ()aeaweb.org/articles?id=10…
Important to think about how to design for both rationing expensive care + encouraging low-cost care. Prior auth is less crude than cost-sharing (I think) because it's mediated by informed docs rather than harried patients; and doesn't require us to sacrifice insurance value.
It does, on the other hand, require real effort by providers and their staff. System-wide savings don't mean that everyone benefits. No way to clear AMA opposition until we solve this problem.
The fact is, providers are the key decision-makers for a lot of care and especially the care we are most worried about overuse of. That suggests we should probably shift incentive provision effort from patients towards them!
OK, there's no way to end a long thread well. So here's a picture of our cats on Halloween.

• • •
Missing some Tweet in this thread? You can try to
force a refresh



