
How much of precision medicine in myeloma is clever marketing, and how much is actual science?
We hear a lot about isatuximab for gain1q and selinexor for del17p!
We unpack all of this in our editorial just published- led by the great hem/onc fellow @OuchveridzeMD
#mmsm
🧵
We hear a lot about isatuximab for gain1q and selinexor for del17p!
We unpack all of this in our editorial just published- led by the great hem/onc fellow @OuchveridzeMD
#mmsm
🧵



Link to study:
sciencedirect.com/science/articl…
1) We start by describing how myeloma is incredibly heterogenous yet treated in a uniform fashion.
There indeed is ample opportunity to treat myeloma in a personalized fashion based on unique features!
sciencedirect.com/science/articl…
1) We start by describing how myeloma is incredibly heterogenous yet treated in a uniform fashion.
There indeed is ample opportunity to treat myeloma in a personalized fashion based on unique features!
Next, we talk about melflufen.
At a ODAC meeting, the sponsor of melflufen tried to tell us that for elderly patients (who represented a very small subset) of patients on the trial, melflufen was better than pomalidomide.
The FDA brilliant response 👇
At a ODAC meeting, the sponsor of melflufen tried to tell us that for elderly patients (who represented a very small subset) of patients on the trial, melflufen was better than pomalidomide.
The FDA brilliant response 👇
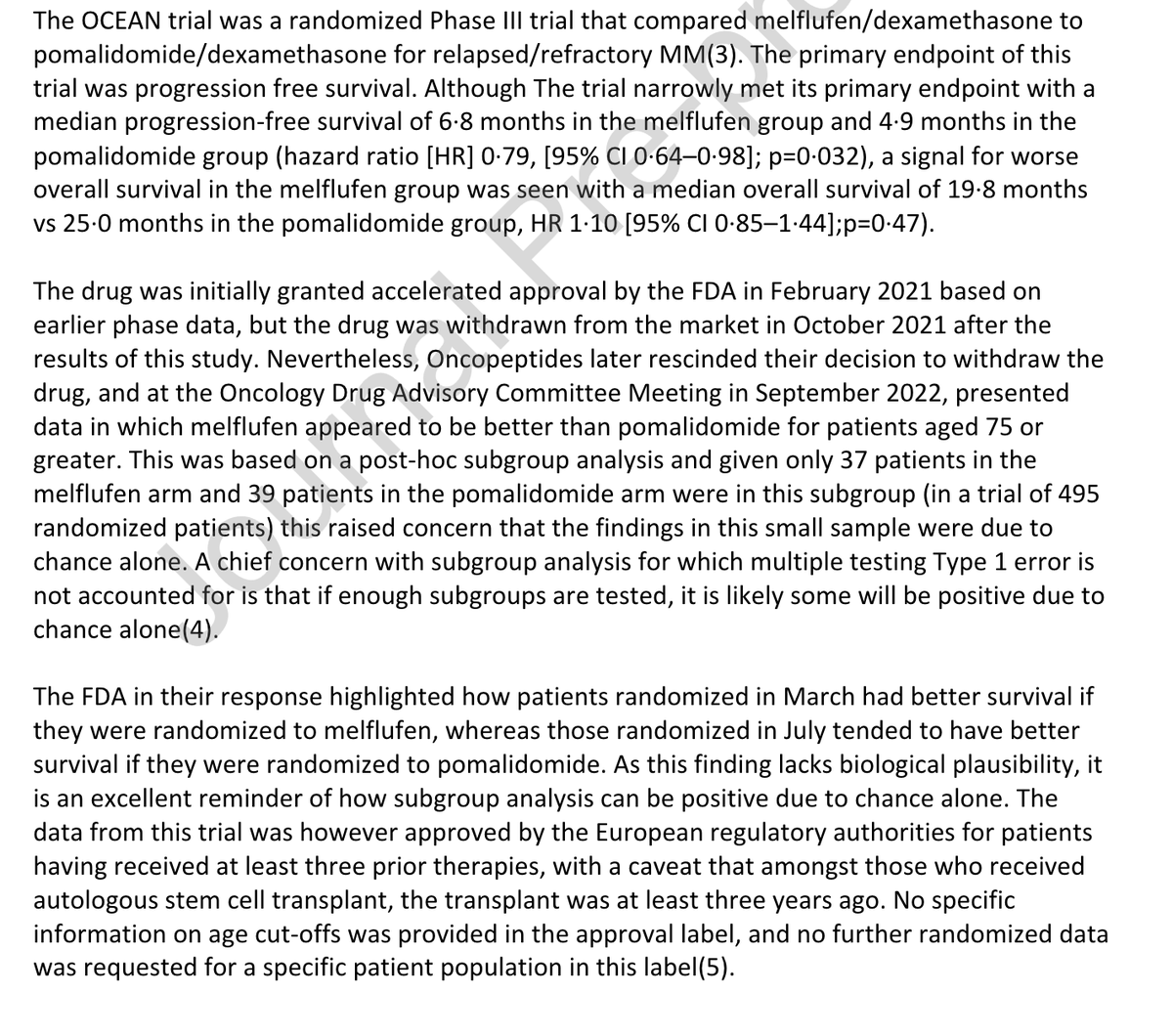
⭐️If you study enough subgroups, it is likely that some will be positive by chance alone. Some will be positive even if they lack any biological plausibility.
The more ways you slice the data and look, the greater risk that some findings are significant because of chance alone
The more ways you slice the data and look, the greater risk that some findings are significant because of chance alone
That said and done- perhaps IMiD's are tough in elderly patients, and benefits attenuated- and this ought to be investigated further. But granting approval based on a subgroup of 76 out of 495 patients?! Further data is needed, and we commend the FDA on their response!
Is selinexor uniquely effective for del17p?
We highlight how Karyopharm markets selinexor as being more effective for p53 "wildtype" in other cancers, and being more effective for p53 mutant/17p deleted myeloma.
How can the same drug with same mechanism of action do that?!
We highlight how Karyopharm markets selinexor as being more effective for p53 "wildtype" in other cancers, and being more effective for p53 mutant/17p deleted myeloma.
How can the same drug with same mechanism of action do that?!

Next- we move on to isatuximab and gain1q. Isatuximab is an unquestionably active/effective drug!
But can we say its uniquely effective in gain1q based on analysis of 3 vs 2 trials?
But what's our null hypothesis? That gain1q wouldn't benefit from addition of a third drug?🧐
But can we say its uniquely effective in gain1q based on analysis of 3 vs 2 trials?
But what's our null hypothesis? That gain1q wouldn't benefit from addition of a third drug?🧐

If we allow industry's marketing agenda of subgroups to prevail, we run the risk of patients receiving treatment on the basis of "multiplicity" rather than biological/clinical efficacy!
We highlight the problematic role oncology news websites such as OncLive play in this issue.
We highlight the problematic role oncology news websites such as OncLive play in this issue.
We end by highlighting solutions:

I thank my friends for their tremendously helpful feedback.
And I thank Chris Booth- a senior author on this paper, who has taught me so much and been a mentor to so many of us including @AaronGoodman33 and @oncology_bg
@rajshekharucms @dgermain21 @HadidiSamer @KUHemOncFellow
And I thank Chris Booth- a senior author on this paper, who has taught me so much and been a mentor to so many of us including @AaronGoodman33 and @oncology_bg
@rajshekharucms @dgermain21 @HadidiSamer @KUHemOncFellow
Also- I must add- we highlight and contrast this to venetoclax- where robust biological data exists, and numerous randomized trials are ongoing to confirm efficacy and safety!

Actual solutions here (wrong screenshot)!
• • •
Missing some Tweet in this thread? You can try to
force a refresh




