One more redo🧵for the students...
Here I will explain what is meant by 'French' when we are talking about Foleys and NG tubes and such.
Also we will cover what the 'Gauge' of an IV means.
(1/ )
Here I will explain what is meant by 'French' when we are talking about Foleys and NG tubes and such.
Also we will cover what the 'Gauge' of an IV means.
(1/ )


'French' isn't named after France 🇫🇷, the country.
It's (indirectly) named after a person -- Joseph-Frédéric-Benoît Charrière, a Swiss instrument maker who started off making knives but went on to make a huge variety of surgical instruments.
It's (indirectly) named after a person -- Joseph-Frédéric-Benoît Charrière, a Swiss instrument maker who started off making knives but went on to make a huge variety of surgical instruments.

When Charrière made instruments, he picked his own unit of measurement that corresponded to 1/3 of a millimeter...this was the 'Charrière'.
But English speakers struggled to pronounce 'Charrière', so the companies changed it to 'French'.
So 1 'French' became 1/3 millimeter.
But English speakers struggled to pronounce 'Charrière', so the companies changed it to 'French'.
So 1 'French' became 1/3 millimeter.


Again: 1 Fr = 1/3 mm.
Only things that are circular tubes have a 'French'. So things like central lines, NG tubes, Foleys, etc.
The 'French' always refers to the *outer diameter* of a tube.
For example, an 18 Fr NG tube = an NG tube with an *outer diameter* of 6 mm.
Only things that are circular tubes have a 'French'. So things like central lines, NG tubes, Foleys, etc.
The 'French' always refers to the *outer diameter* of a tube.
For example, an 18 Fr NG tube = an NG tube with an *outer diameter* of 6 mm.

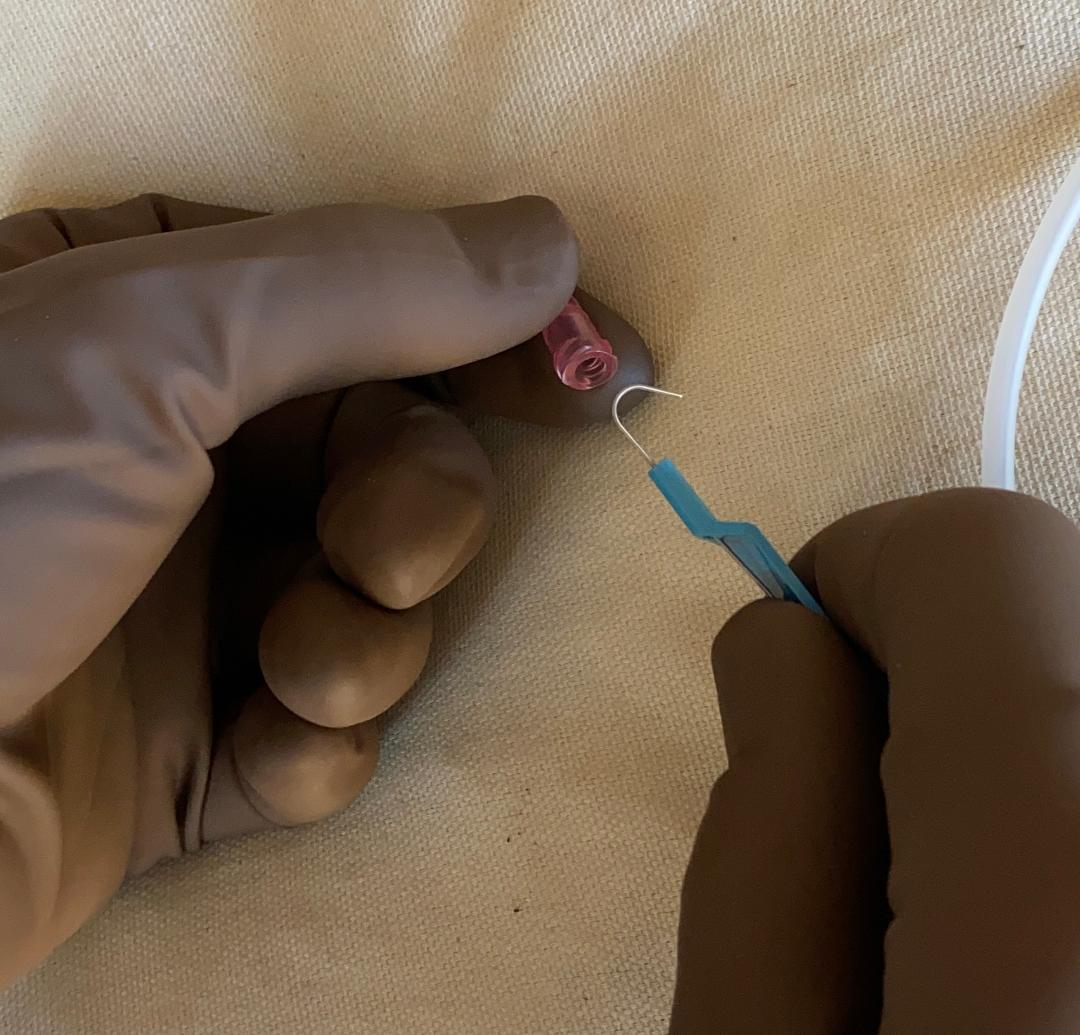
Here is a 7 Fr central line (triple lumen).
Again, the '7 Fr' refers to the *outer diameter*. It doesn't matter how many lumens it may have: that's a separate issue. It's 7 Fr, and therefore its outer diameter is 7/3 = 2.33 mm.
Again, the '7 Fr' refers to the *outer diameter*. It doesn't matter how many lumens it may have: that's a separate issue. It's 7 Fr, and therefore its outer diameter is 7/3 = 2.33 mm.


It's the same unit of measurement for all devices:
A 12 Fr NG tube has the same outer diameter as a 12 Fr dialysis catheter, a 12 Fr Foley catheter, or a 12 Fr chest tube.
All of these 12 Fr devices will have an outer diameter of 12/3 = 4 mm.
A 12 Fr NG tube has the same outer diameter as a 12 Fr dialysis catheter, a 12 Fr Foley catheter, or a 12 Fr chest tube.
All of these 12 Fr devices will have an outer diameter of 12/3 = 4 mm.




In some countries that have less of a problem pronouncing 'Charrière', catheters instead use the 'Ch' abbreviation instead of 'French'.
Here we see an '18 Ch' Foley, and we are reminded again that this means it's 6 mm in diameter.
Here we see an '18 Ch' Foley, and we are reminded again that this means it's 6 mm in diameter.

On the other hand 'Gauge' is a different thing entirely.
'Gauge' refers to the Birmingham Gauge system, devised in the 1900's in England for manufacturing metal wire. It later became used for IV catheters.
There are a couple of major differences...
'Gauge' refers to the Birmingham Gauge system, devised in the 1900's in England for manufacturing metal wire. It later became used for IV catheters.
There are a couple of major differences...

First, as the 'Gauge' number gets *larger*, the IV's get *smaller*. This is the opposite of the 'French' system.
As you can see here, a 14 Fr IV catheter is much larger than a 24 Fr catheter.
As you can see here, a 14 Fr IV catheter is much larger than a 24 Fr catheter.

Also the 'Gauge' sizes are somewhat arbitrary...meaning the spacing isn't mathematically consistent.
So a 10 Gauge IV is *not* twice the size of a 20 Gauge IV, for example.
If you do the math here, you see these relationships are not linear or consistent.
So a 10 Gauge IV is *not* twice the size of a 20 Gauge IV, for example.
If you do the math here, you see these relationships are not linear or consistent.

Finally, as a trauma surgeon, I have to point out one of my favorite teaching points:
The flow rate of a 16 G IV is **twice** that of an 18 G IV. So the difference between those two IV's may not sound much at first, but it makes a big difference for major resuscitations...
⬛️
The flow rate of a 16 G IV is **twice** that of an 18 G IV. So the difference between those two IV's may not sound much at first, but it makes a big difference for major resuscitations...
⬛️

Of course I have a critical typo in my most-read 🧵😬😤😫
As the picture indicates, these IV's are expressed in terms of "Gauge". A couple of slides ago, I accidentally used the wrong abbreviation in the text.
As the picture indicates, these IV's are expressed in terms of "Gauge". A couple of slides ago, I accidentally used the wrong abbreviation in the text.

Also, not to complicate things, but some have pointed out that there’s an exception for vascular access sheaths.
Here the companies have chosen to use “French” to indicate the size of the things that can pass through them.
In this case the outer diameter will be larger 🤔.
Here the companies have chosen to use “French” to indicate the size of the things that can pass through them.
In this case the outer diameter will be larger 🤔.
https://twitter.com/pauldevlinmd/status/1618667960444530694
• • •
Missing some Tweet in this thread? You can try to
force a refresh