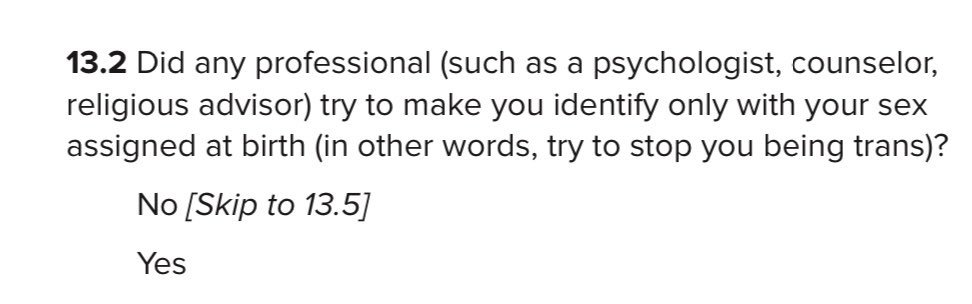
Due to the ideological capture of our institutions, the search for studies based on sound methodology on topics related to Gender Affirming Care can be futile. Many of these flawed studies have also been challenged & discredited. I’ll link some resources in this 🧵. Pls save.
https://twitter.com/TheRealDHR/status/1629352836504100865
@mr_ryan_head @TheRealDHR, apologies for permanently linking you to my pinned tweet. I hope it hasn’t caused you too much trouble.
• • •
Missing some Tweet in this thread? You can try to
force a refresh