Proud to contribute to the remarkable scientific journey of #APT, whose 10-year analysis is now published on @TheLancetOncol. Adjuvant TH confirmed outstanding long-term outcomes for patients with small HER2+ breast cancer. Aim for the next decade: biomarker-informed treatments! 
https://twitter.com/stolaney1/status/1630557281787219968

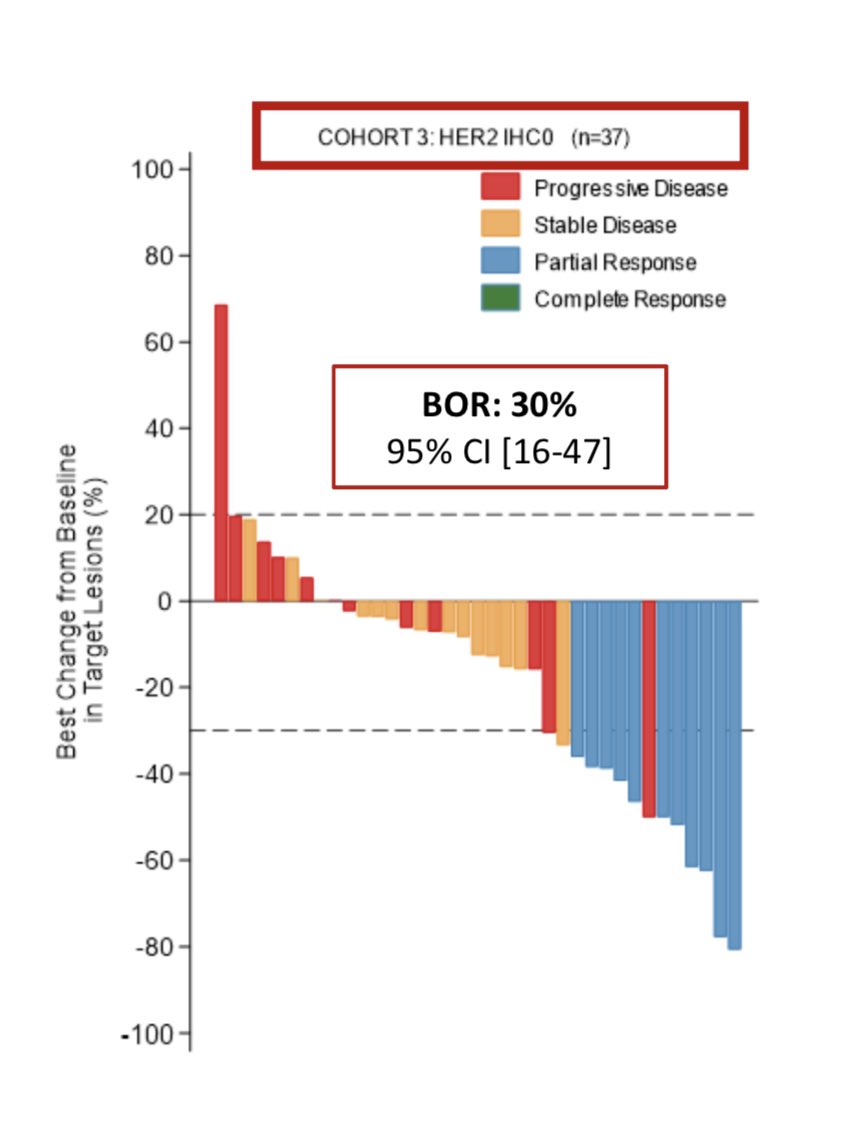
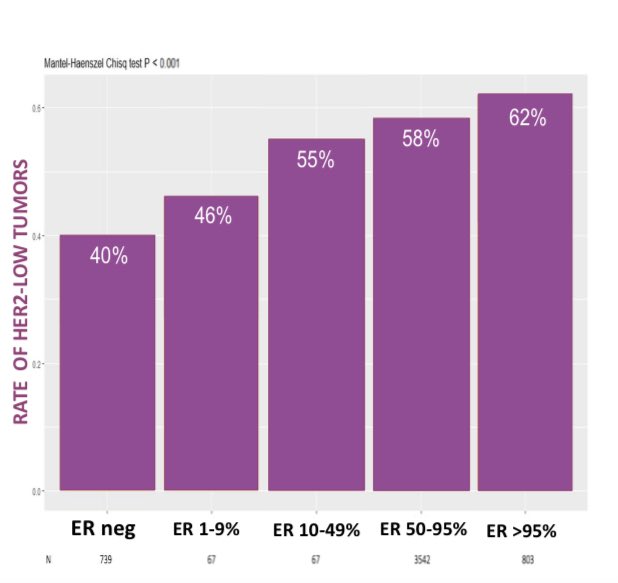
Here a thread on the clinical and biomarker findings from this 10-year update: 👇 🧵
https://twitter.com/prat_aleix/status/1630455898253451265
Icing on the cake: a great accompanying commentary by Elena Geuna, @curijoey & @FilippoMontemu1
sciencedirect.com/science/articl…
sciencedirect.com/science/articl…
A thousand thanks to @stolaney1 for making this practice changing work possible and for being a constant source of inspiration, to the @RevealGenomics team for the partnership that helped learning from the samples, and to all the patients and researchers involved in this trial.
• • •
Missing some Tweet in this thread? You can try to
force a refresh