
#HGESummit Day 2 thoughts below🧵⬇️
Starting with an exhibit at @TheCrick asking visitors for their perspectives on gene editing. The range of responses shows the need to keep having these tough conversations - with everyone who has a stake in the discussion.
Starting with an exhibit at @TheCrick asking visitors for their perspectives on gene editing. The range of responses shows the need to keep having these tough conversations - with everyone who has a stake in the discussion.




(2/🧵) I wish I had enough characters for all of @BettinaRyll ‘s comments about communities’ roles in setting research agendas. I’ll pick one that resonated deeply - “Scientists are part of civil society, too.”
#HGESummit 🧬
#HGESummit 🧬
One more, because @BettinaRyll ‘s message was so powerful, “if our model systems are homogenous cell cultures kept in plastic dishes, we shouldn’t be surprised that our translational gap is so large.” Patients are people, not model organisms.
#HGESummit 🧬
#HGESummit 🧬
I’ll admit that the term “biohacker” also made me think of “wild, unregulated research” - @lexikon1 is making me rethink biohackers’ role as active participants who bridge the gap between unmet community needs and research agendas that prioritize them.
#HGESummit 🧬
#HGESummit 🧬
@lexikon1 “researchers are de-incentivized from publishing in open access journals” due to the high cost - especially if they don’t have backing from a large institution. Science has suffered from a lack of transparency - but Open Access leaves others behind.
#HGESummit 🧬
#HGESummit 🧬
Gene editing won’t be therapeutic without a reliable way to deliver the therapy to the right cells, at the right time. @jonirutter shares how platform-based approaches can help future therapies reach their targets while accelerating the approval process.
#HGESummit 🧬
#HGESummit 🧬
Two fun facts about @CaribouBio ‘s next-gen chRDNA guide technology:
1. Using an RNA-DNA hybrid (instead of traditional RNA) as a guide increases gene specificity and decreases off-target editing.
2. “ChRDNA” is pronounced “Chardonnay” - a choice I can get behind.
#HGESummit 🧬
1. Using an RNA-DNA hybrid (instead of traditional RNA) as a guide increases gene specificity and decreases off-target editing.
2. “ChRDNA” is pronounced “Chardonnay” - a choice I can get behind.
#HGESummit 🧬
Sonja Schrepfer brings up a point I hadn’t thought about - fetuses are “allogeneic” by way of expressing paternal proteins, and studying their tolerance during pregnancy could reveal ways to protect engineered cells from the host’s immune system.
#HGESummit 🧬
#HGESummit 🧬
The gap between “what science can do” and “what patients need most” has been a recurring theme. It’s a lot easier to talk about success stories than hard challenges - what happens when patient populations aren’t seen as “profitable”?
#HGESummit 🧬
#HGESummit 🧬
Re-upping @MelissaSCreary’s quote from yesterday in relation to today’s session on Accessibility and Price: “patients’ bodies are treated as commodities in the research community.”
#HGESummit 🧬
#HGESummit 🧬
Don’t forget about the epigenome! Angelo Lombardo shows proof-of-concept for gene silencing via persistent epigenetic modifications.
#HGESummit 🧬
#HGESummit 🧬
@UrnovFyodor picks up this morning’s accessibility and price conversation with his “most important slide” describing a non-viral, “plug-and-play” platform that could streamline R&D and regulatory processes while reducing cost.
#HGESummit 🧬
#HGESummit 🧬

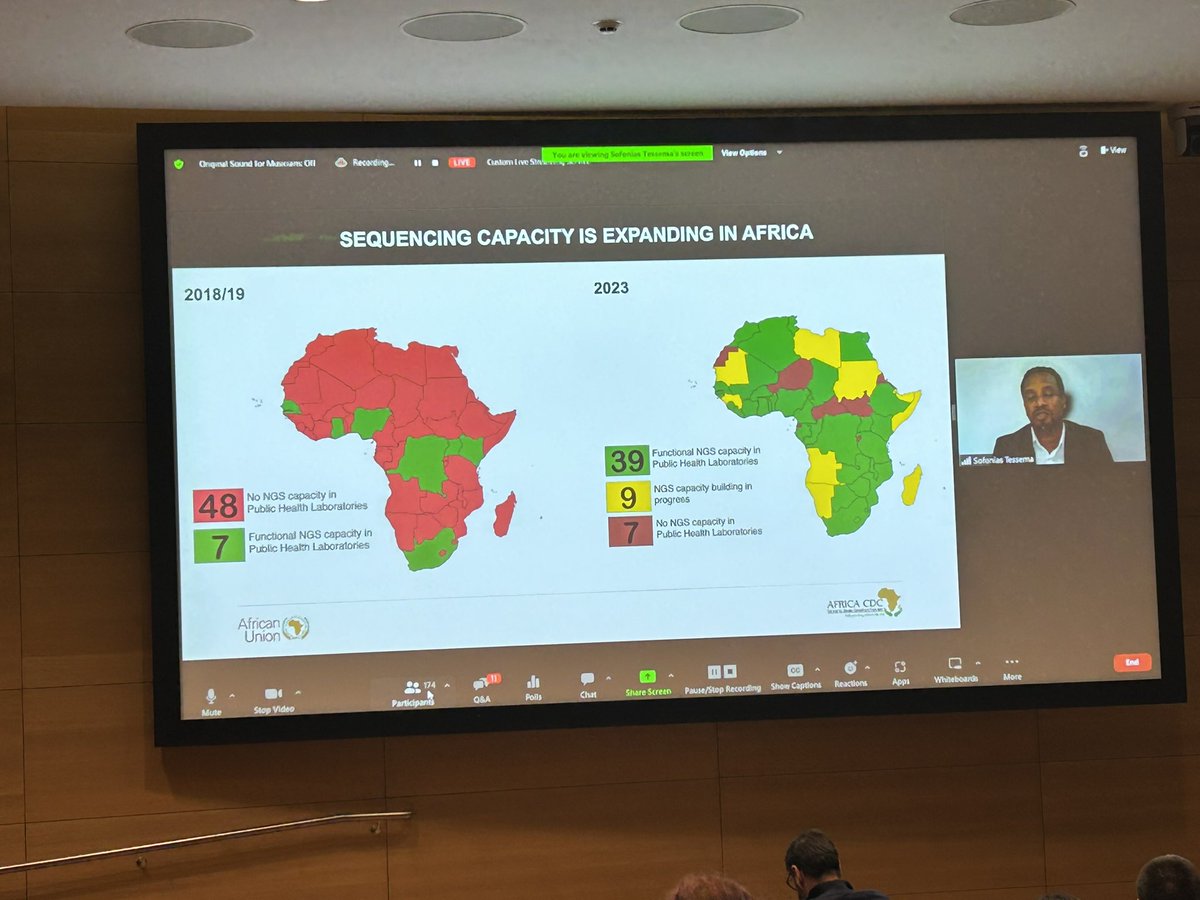
Diagnostic sequencing is “cheap and easy” for many of the researchers here, which is not the case globally. @sofoniaskt shares work to expand next-gen sequencing capacity in Africa.
#HGESummit 🧬
#HGESummit 🧬
Katherine Littler of @WHO says “If I don’t leave you with the fact that our governance has to be just as dynamic as our science, then I have failed.”
#HGESummit 🧬
#HGESummit 🧬
Speaking on the need to incorporate (largely uncatalogued) variants from low and middle income countries in gene therapy development, @kiranmusunuru says “I have to do better, and we all have to do better, starting now.”
#HGESummit 🧬
#HGESummit 🧬
• • •
Missing some Tweet in this thread? You can try to
force a refresh





