1/5
Check out the two CBCs in the graphic.
QUESTION: Do either/both of these patients have anisocytosis?
NOTE: RDW-CV and RDW-SD are discordant.
Check out the two CBCs in the graphic.
QUESTION: Do either/both of these patients have anisocytosis?
NOTE: RDW-CV and RDW-SD are discordant.

2/5
MCV represents the average volume of RBCs measured, but does not provide information about variation in cell size.
The latter can be estimated by measuring the diameter of many RBCs under the light microscope. More commonly it is generated as the RDW by automated counters.
MCV represents the average volume of RBCs measured, but does not provide information about variation in cell size.
The latter can be estimated by measuring the diameter of many RBCs under the light microscope. More commonly it is generated as the RDW by automated counters.

3/5
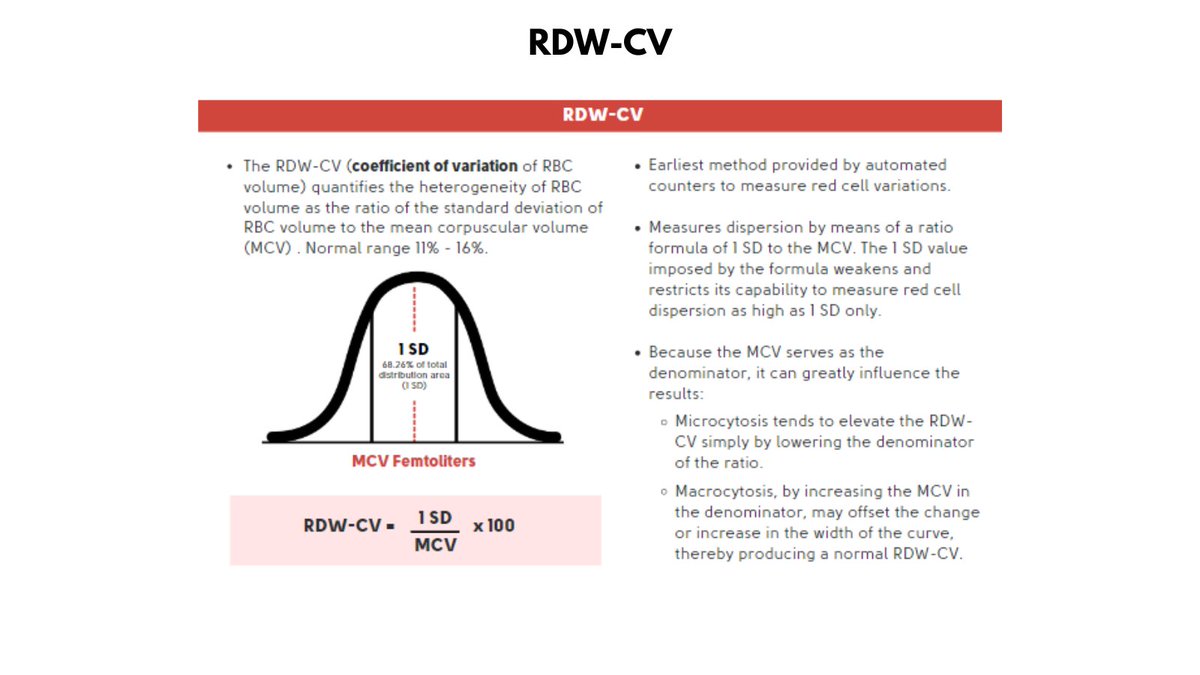
2 ways to express the RDW:
1. RDW-CV is a percentage of the SD/MCV, thus the lower the MCV, the higher the RDW-CV. Conversely, the higher the MCV, the lower the RDW-CV.
2 ways to express the RDW:
1. RDW-CV is a percentage of the SD/MCV, thus the lower the MCV, the higher the RDW-CV. Conversely, the higher the MCV, the lower the RDW-CV.
4/5
2. The RDW-SD is a direct measurement of variation in cell volume, and is not influenced by cell size. Thus, it is a better marker for anisocytosis.
Patient A does not have anisocytosis despite the high RDW-CV.
Patient B has anisocytosis despite the normal RDW-CV.
2. The RDW-SD is a direct measurement of variation in cell volume, and is not influenced by cell size. Thus, it is a better marker for anisocytosis.
Patient A does not have anisocytosis despite the high RDW-CV.
Patient B has anisocytosis despite the normal RDW-CV.

5/5
EASY TO REMEMBER:
a. RDW-SD > 46 fL = anisocytosis
b. A lower than normal RDW-SD is clinically meaningless - lower values reflect less biological noise.
For more info see:
thebloodproject.com/red-blood-cell…
EASY TO REMEMBER:
a. RDW-SD > 46 fL = anisocytosis
b. A lower than normal RDW-SD is clinically meaningless - lower values reflect less biological noise.
For more info see:
thebloodproject.com/red-blood-cell…
• • •
Missing some Tweet in this thread? You can try to
force a refresh