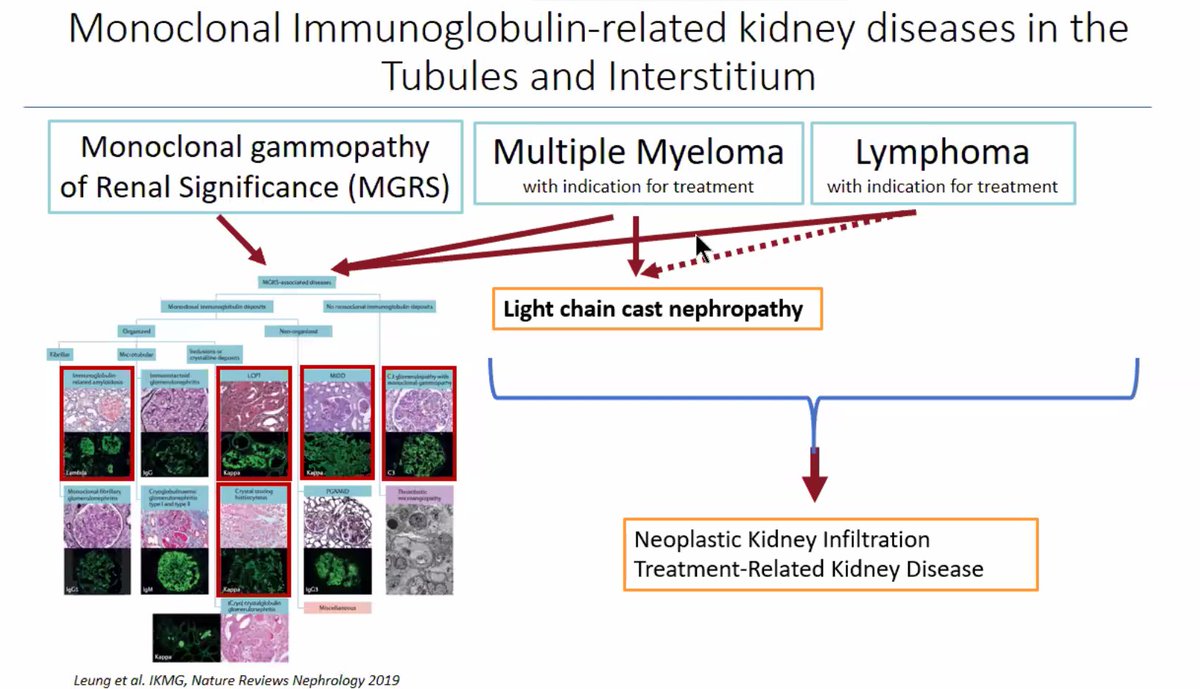
Dr. Virginie Royal gave a beautiful overview of diseases of monoclonal immunoglobulin deposition involving the tubulointerstitum.
Here are some pearls:
Here are some pearls:
Clinical presentations can be variable, but often include proteinuria +/- AKI, as well as evidence of tubular dysfunction (including Fanconi syndrome).

Light chain deposition disease is characterized by the deposition of light chains along tubular basement membranes, glomerular basement membranes, and throughout the interstitium.


There are rare cases of LCDD that lack glomerular involvement.
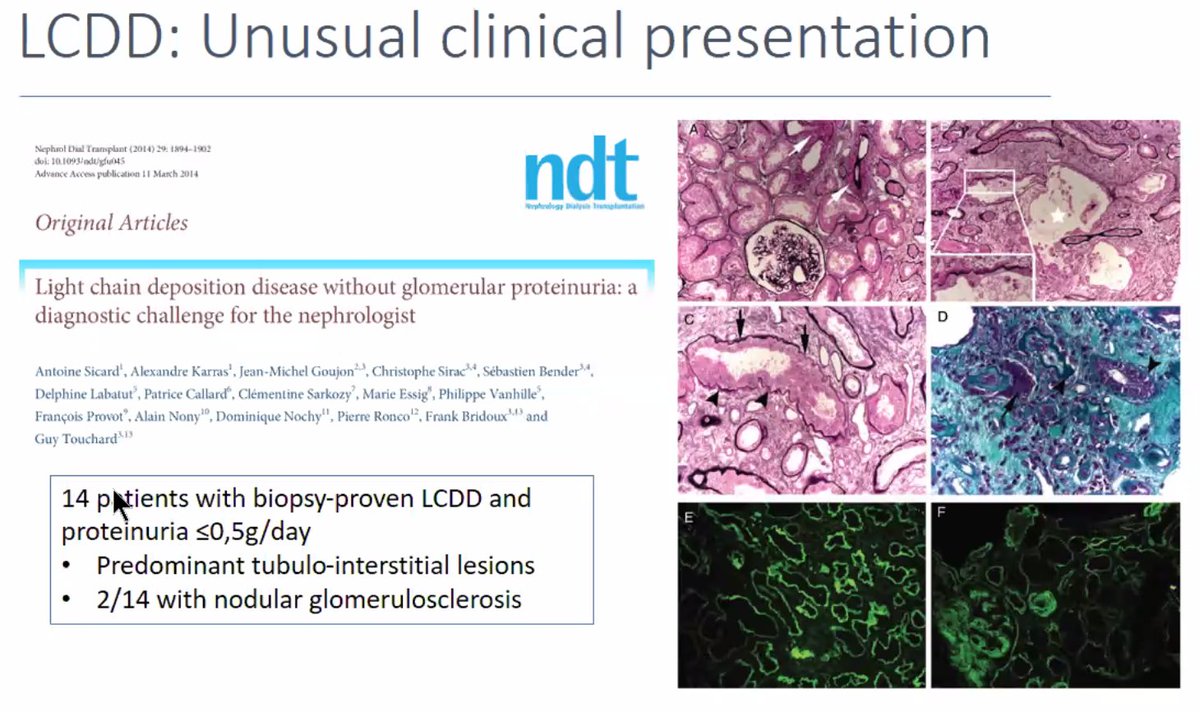
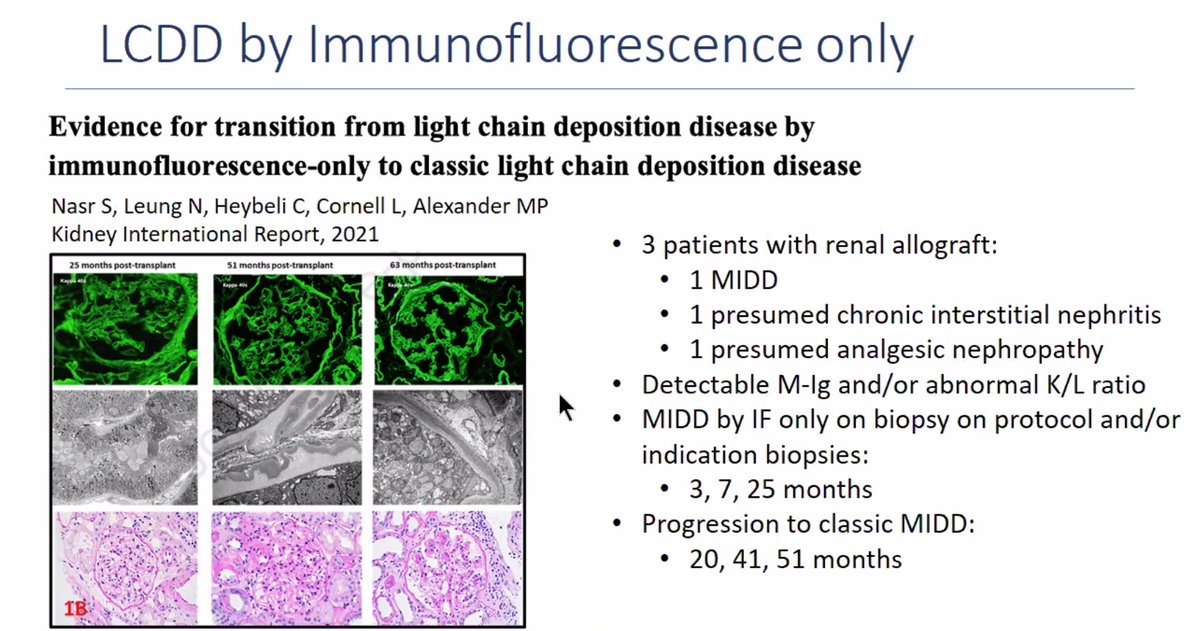
In LCDD, you often see powdery light chain deposits ultrastructurally, but early in the disease you may have LCDD by immunofluorescence only, which can later progress to demonstrating 'classic' deposits.
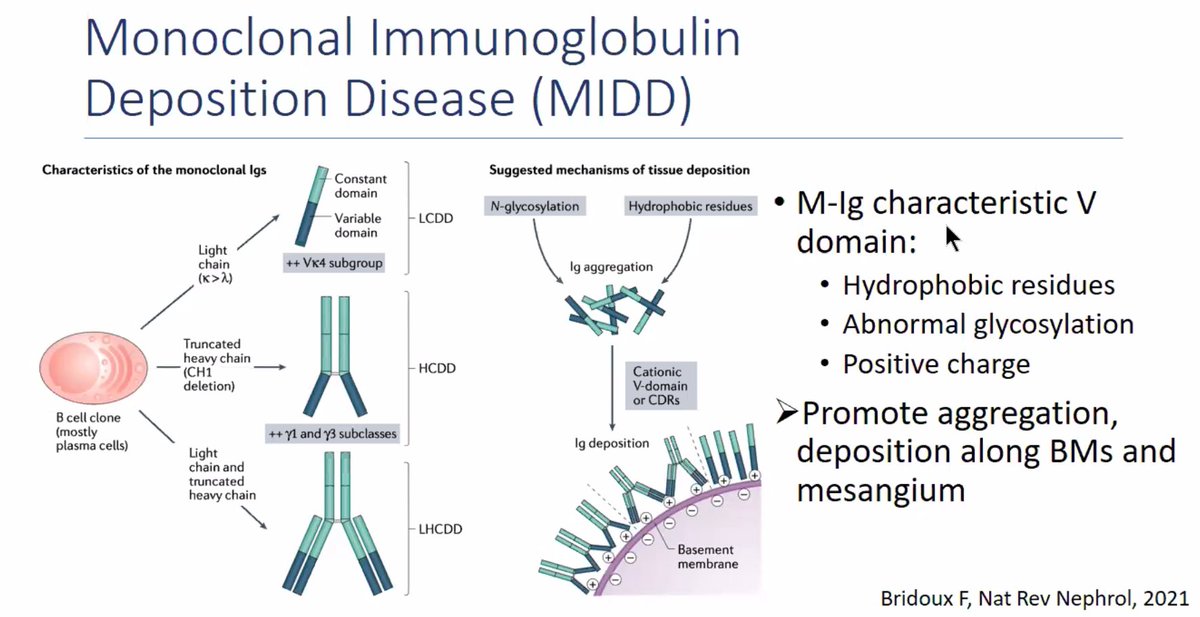
Proposed mechanism for LCDD:
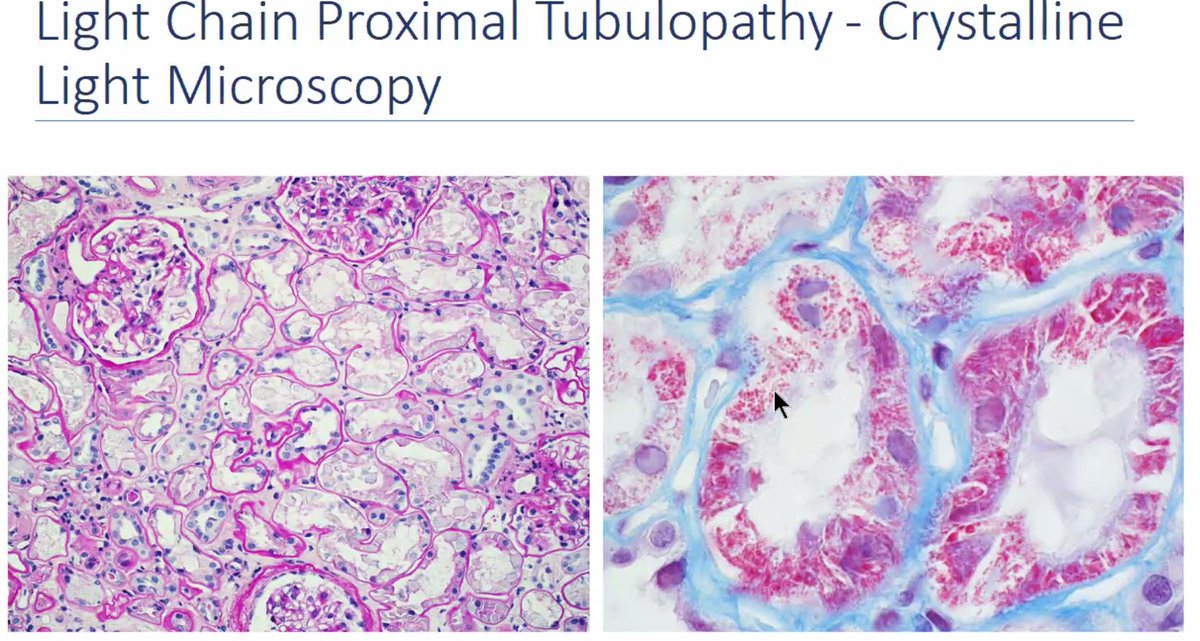
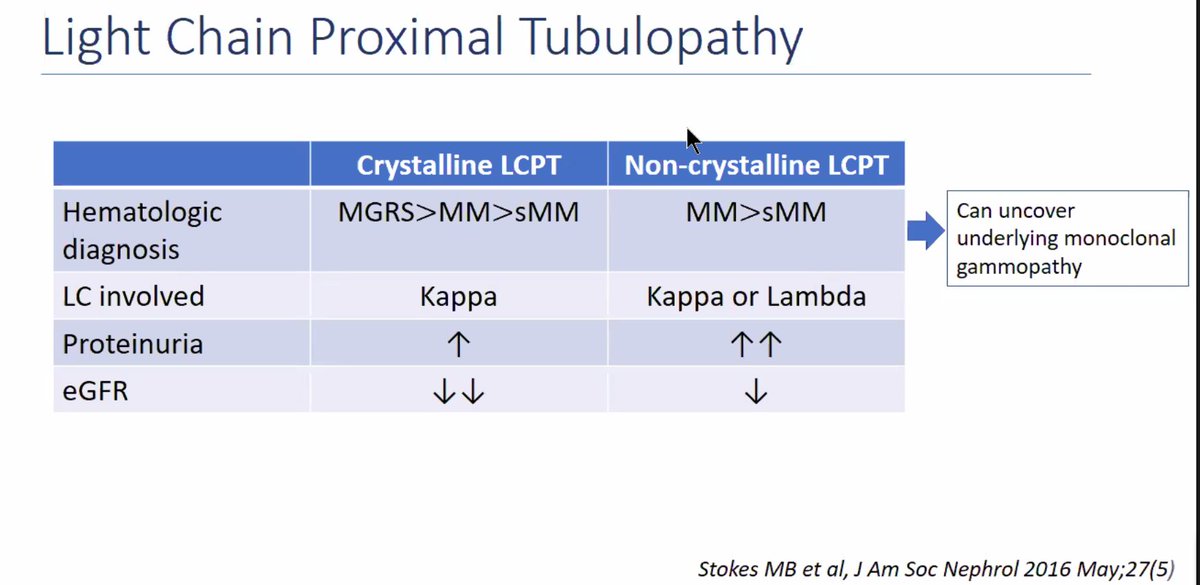
Light chain proximal tubulopathy is another MRGS lesion of the tubulointerstitium. It has both crystalline and non-crystalline forms.

Light chain proximal tubulopathy with crystals shows PAS-pale and fuschinophilic inclusions within proximal tubules.
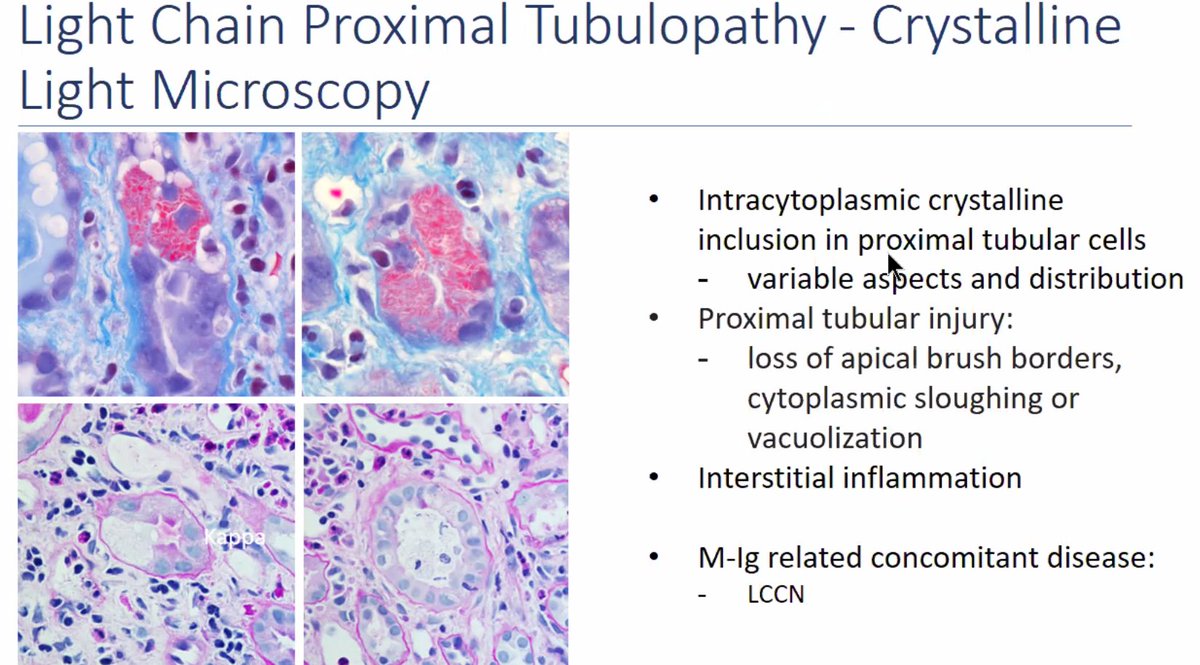
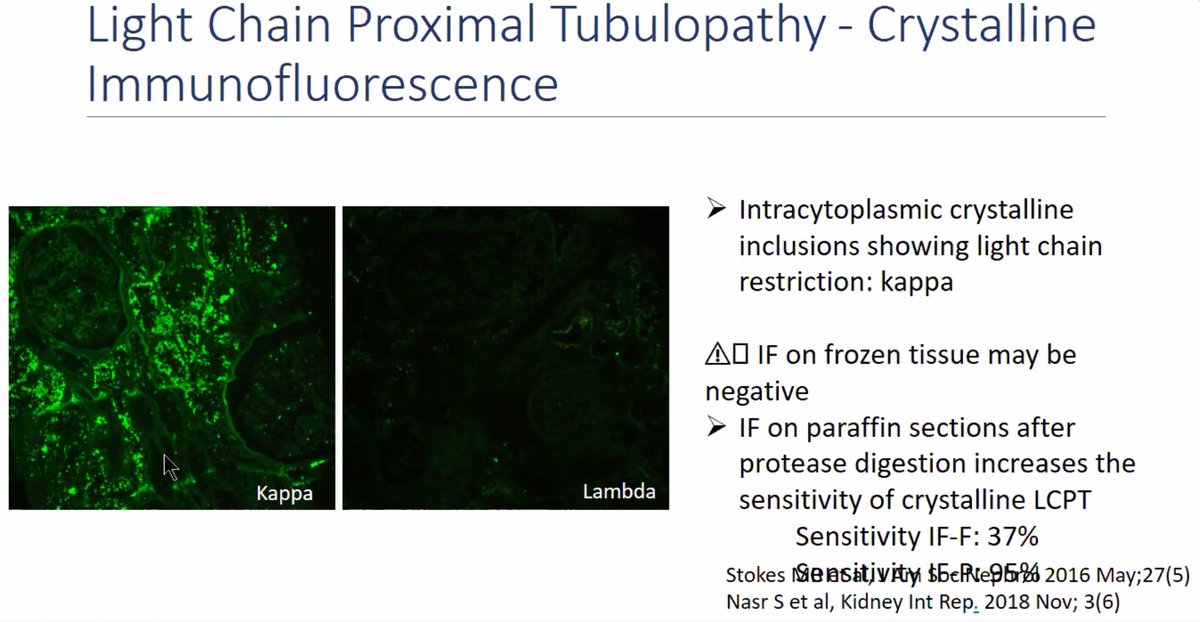
LCPT with crystals may show 'masking' by routine immunofluorescence and require pronase retrieval/paraffin immunofluorescence to demonstrate light chain restriction.
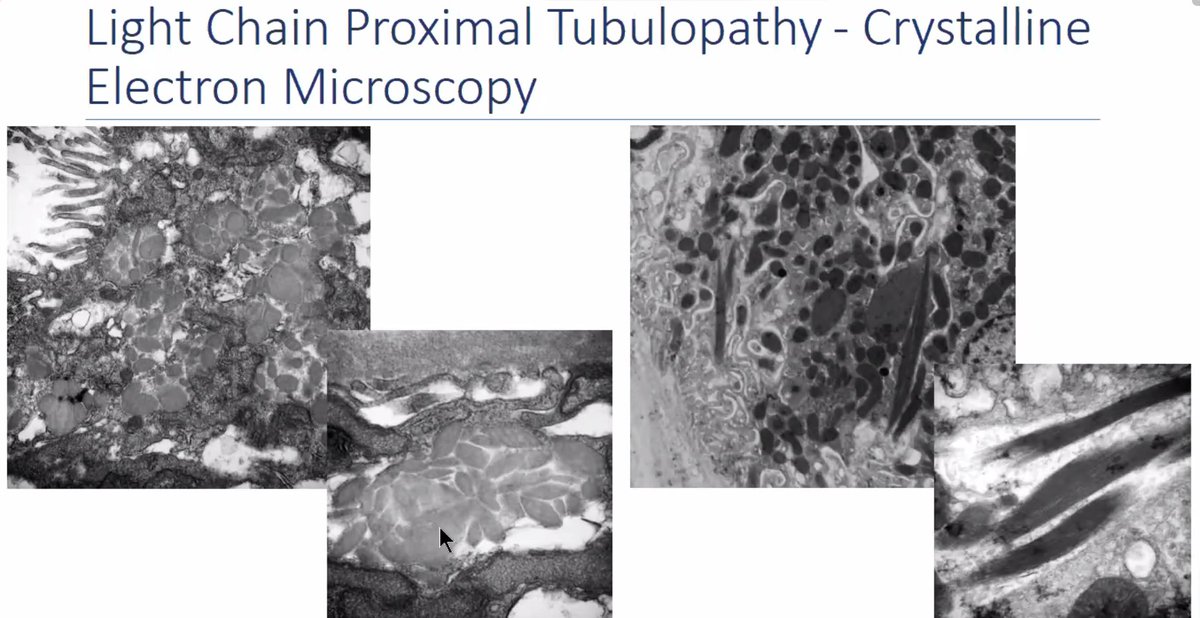
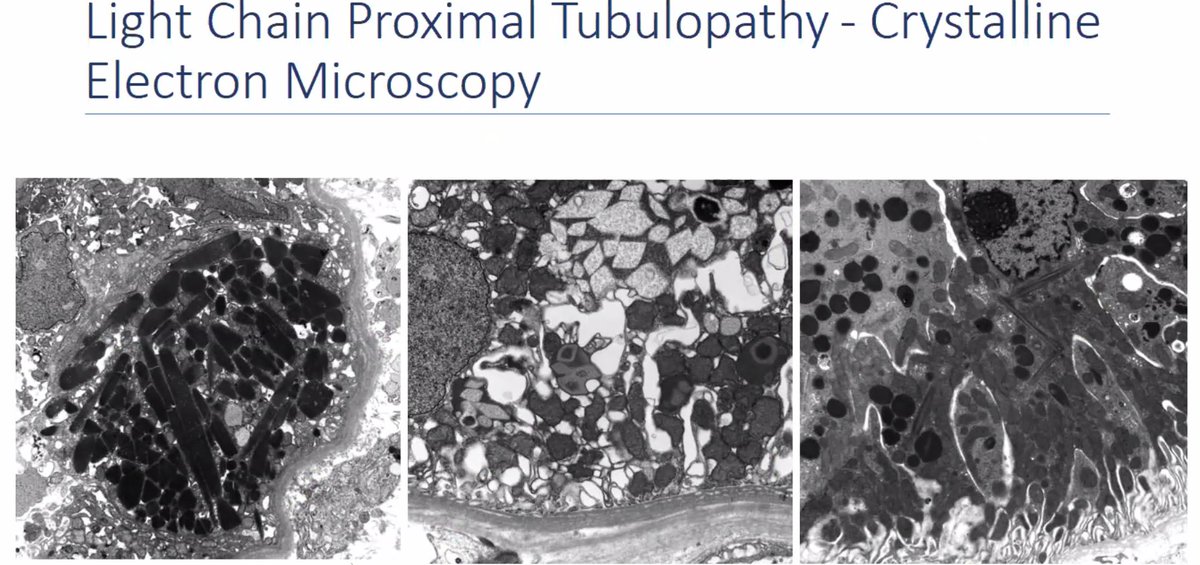
Crystalline inclusions in LCPT with crystals show variable morphology.
LCPT without crystals shows light chain restriction within proximal tubules, without presence of crystals, but with abundant phagolysosomes in proximal tubules, which can give a 'bubbly' appearance by light microscopy.

Crystalline LCPT is almost always kappa light chain. For the non-crystalline variant, the specificity can be either kappa or lambda and the differential diagnosis includes trafficking of free light chains, so establishing end-organ damage due to the monoclonal Ig is important
Crystal-storing histiocytosis and light chain podocytopathy are exceedingly rare MGRS lesions, with similar light chain precipitation/crystal formation.

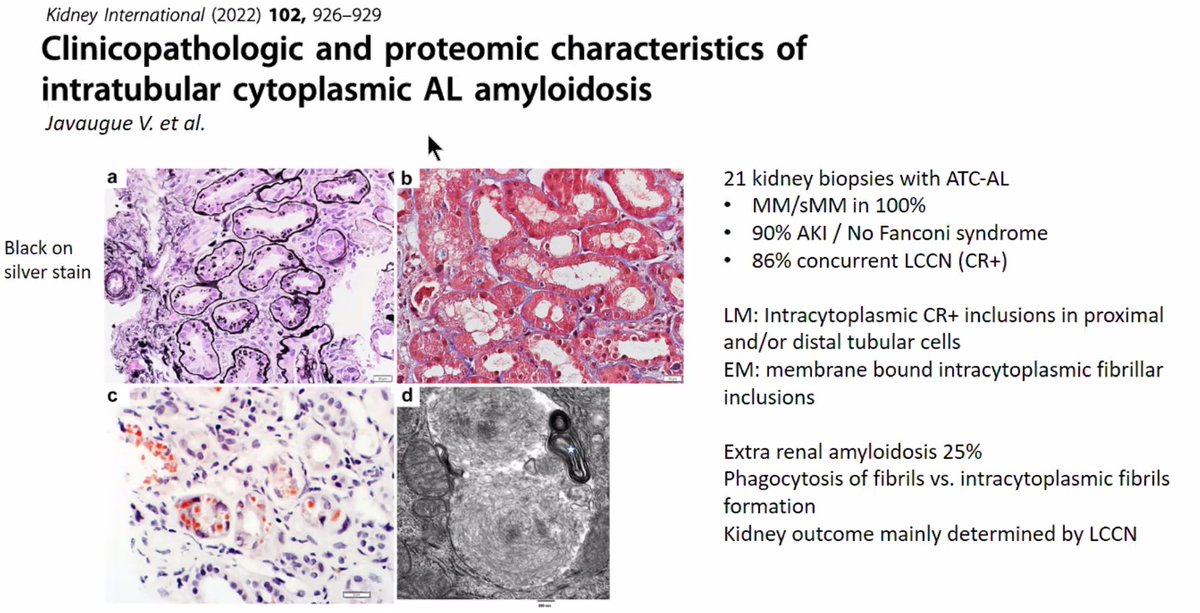
Intratubular amyloid can appear like light chain proximal tubulopathy, which is a form of AL amyloidosis. It is highly associated with multiple myeloma and frequently occurs concurrently with light chain cast nephropathy.
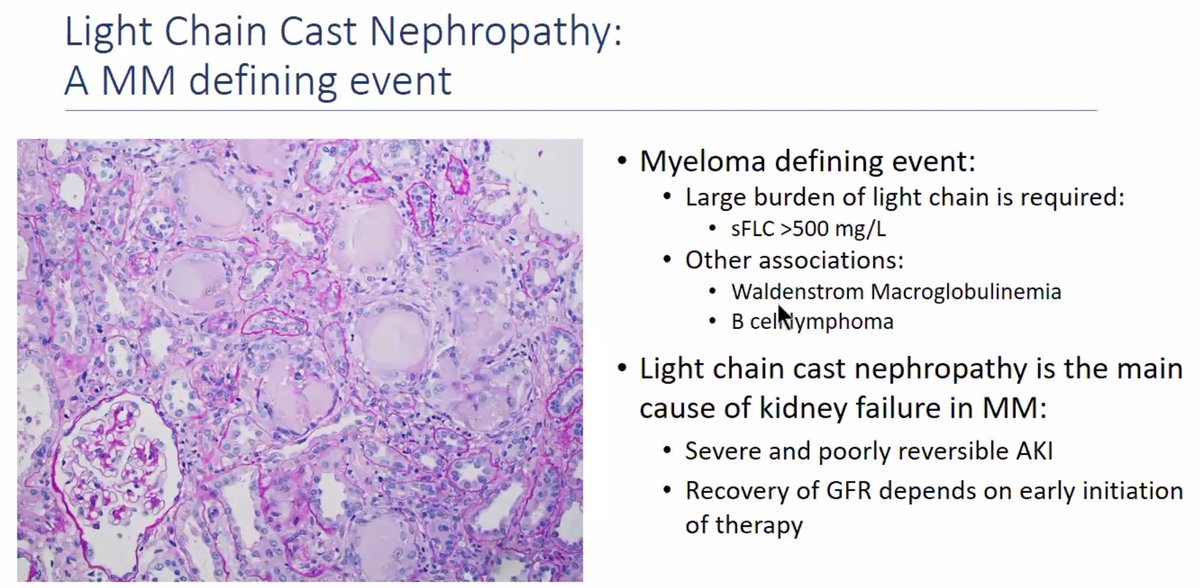
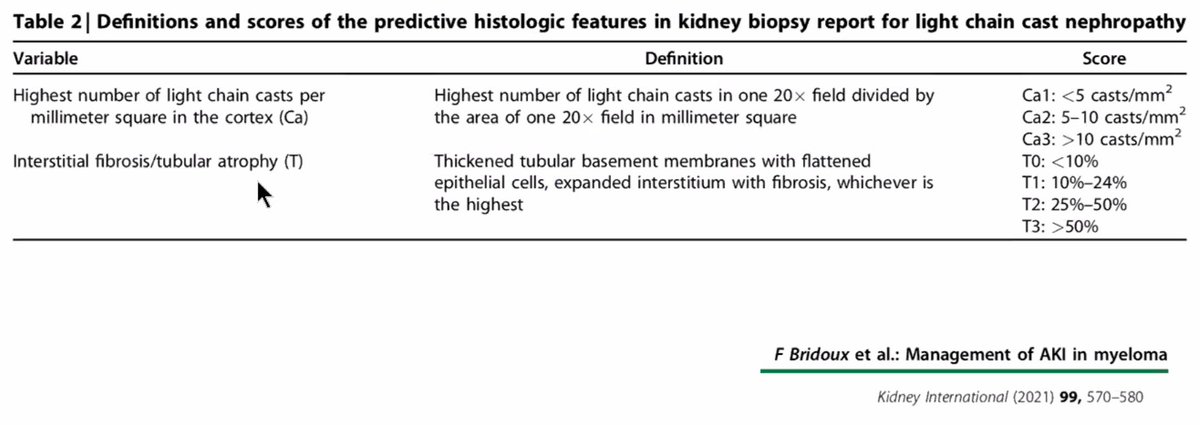
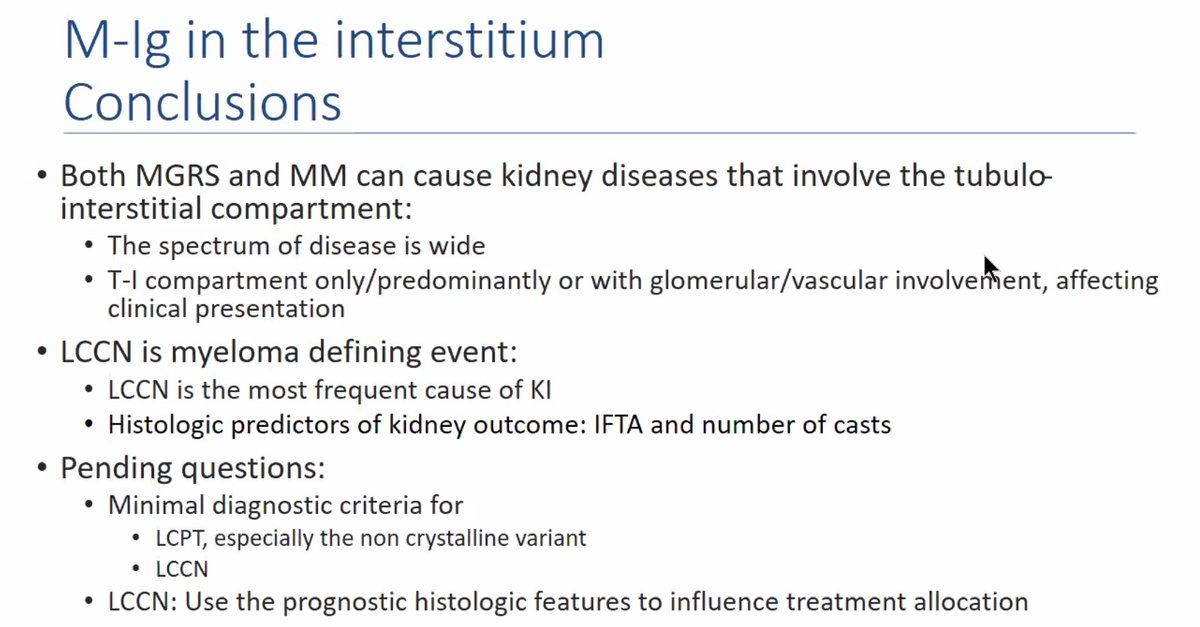
Light chain cast nephropathy is not considered a MGRS lesion, but is a myeloma defining event.
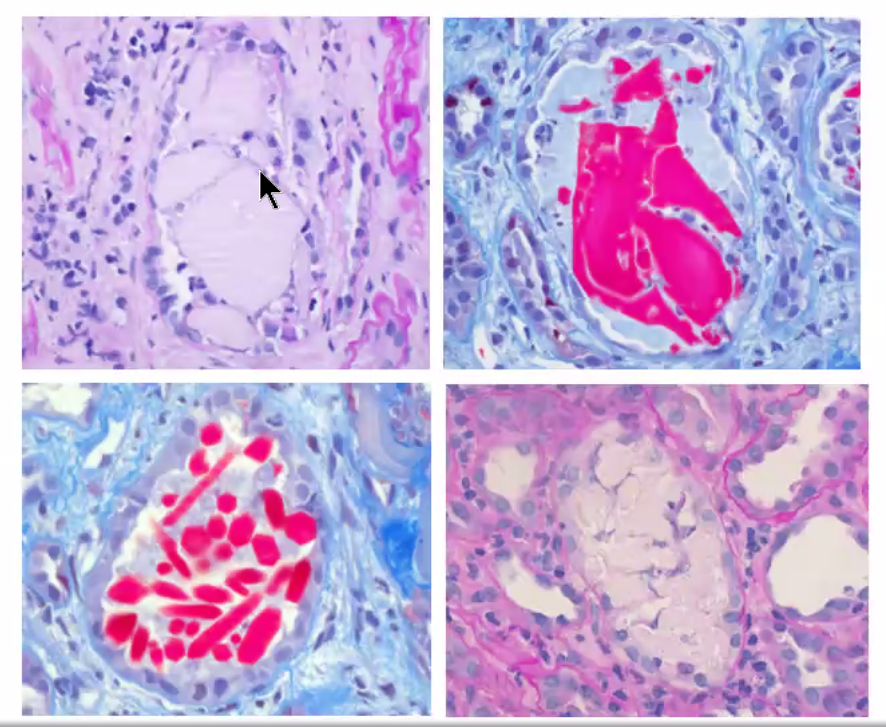
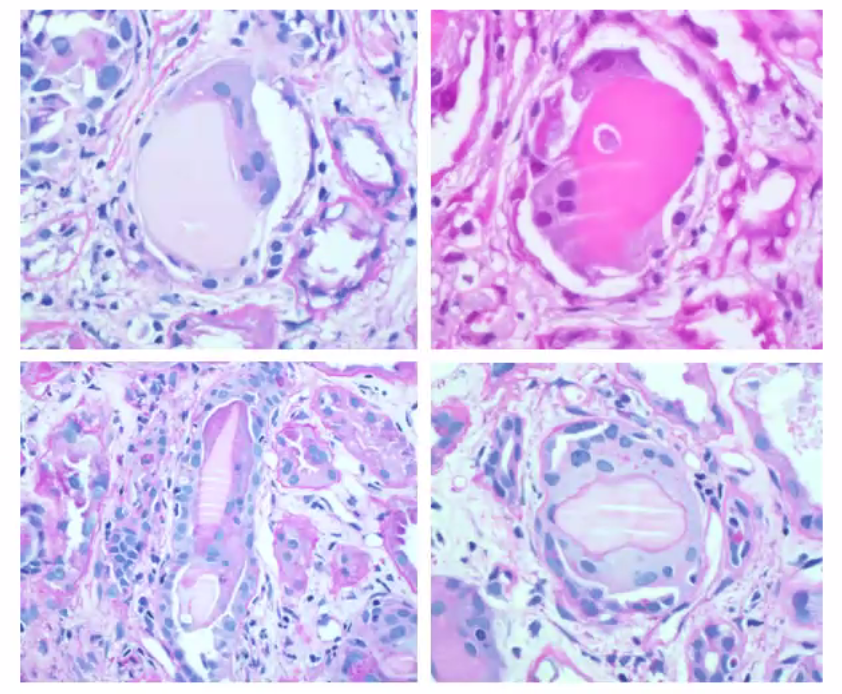
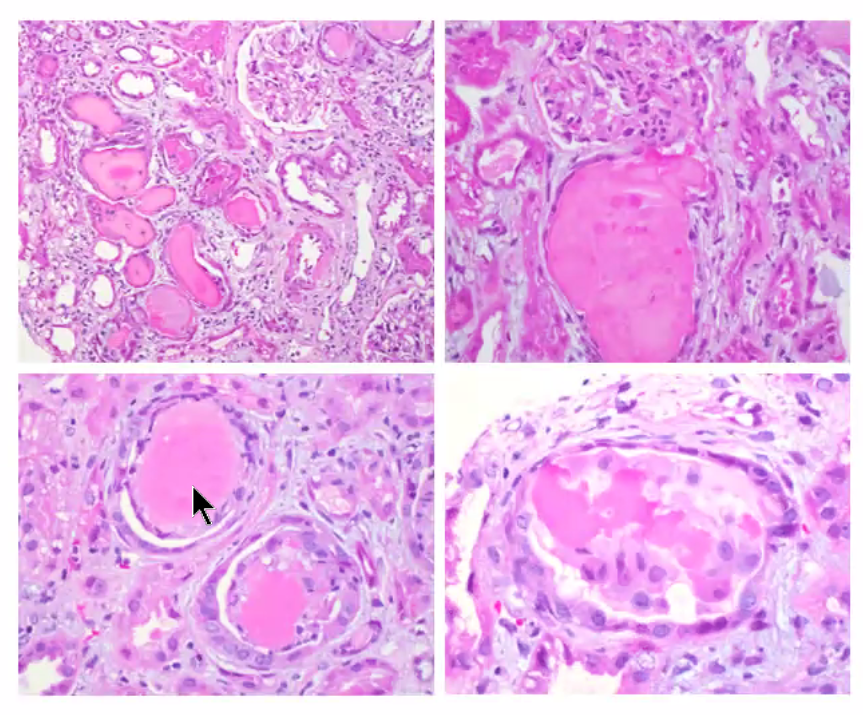
Morphologic features of light chain casts:
1. PAS pale
2. Fractured or crystalline
3. Cellular reaction (can be giant cell)
1. PAS pale
2. Fractured or crystalline
3. Cellular reaction (can be giant cell)
Challenges in diagnosing light chain cast nephropathy and ancillary studies which may prove helpful:
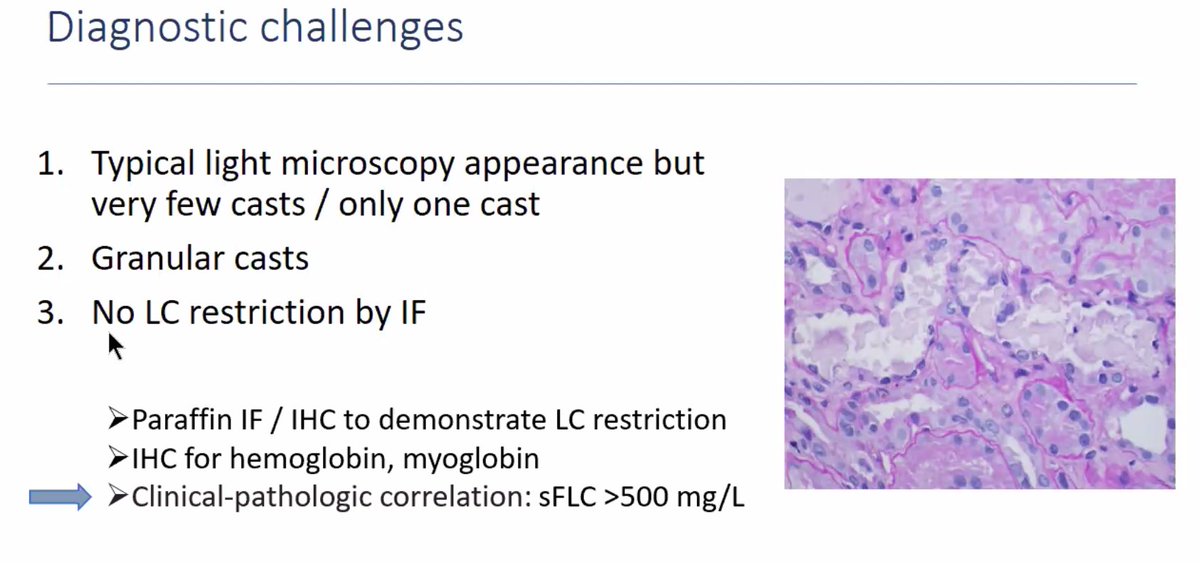
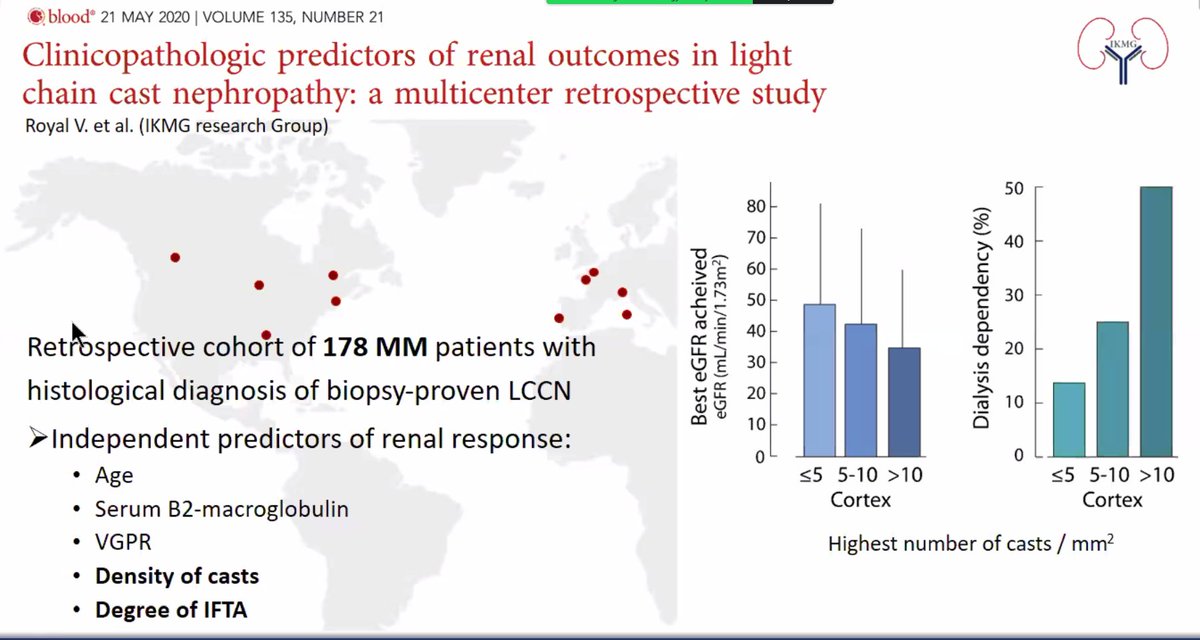
Only one light chain restricted cast is required for a diagnosis of light chain cast nephropathy, however, a large cast burden is associated with a poor renal prognosis.
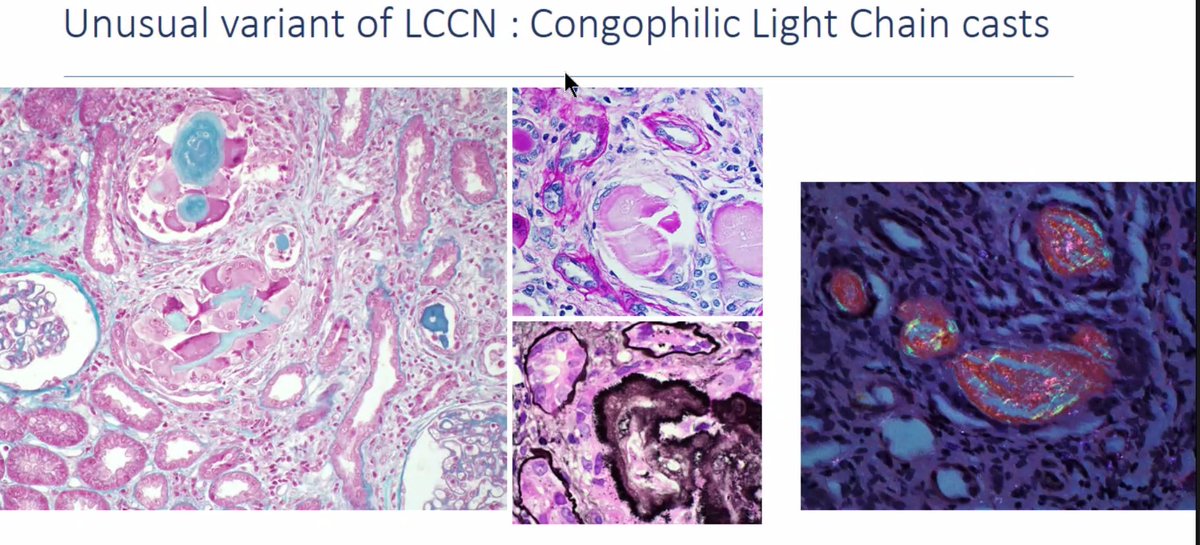
Light chain casts can stain positive for Congo red. These cases may be associated with systemic AL amyloidosis.
Light chain amyloidosis (AL) or heavy/light chain amyloidosis (AHL) can involve all renal compartments.
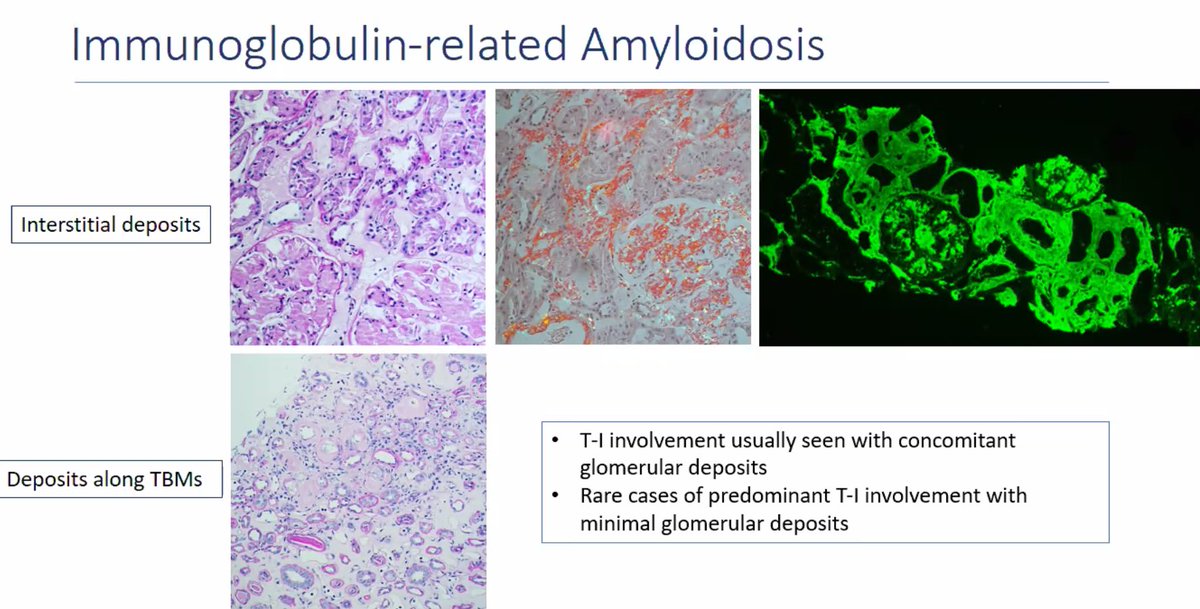
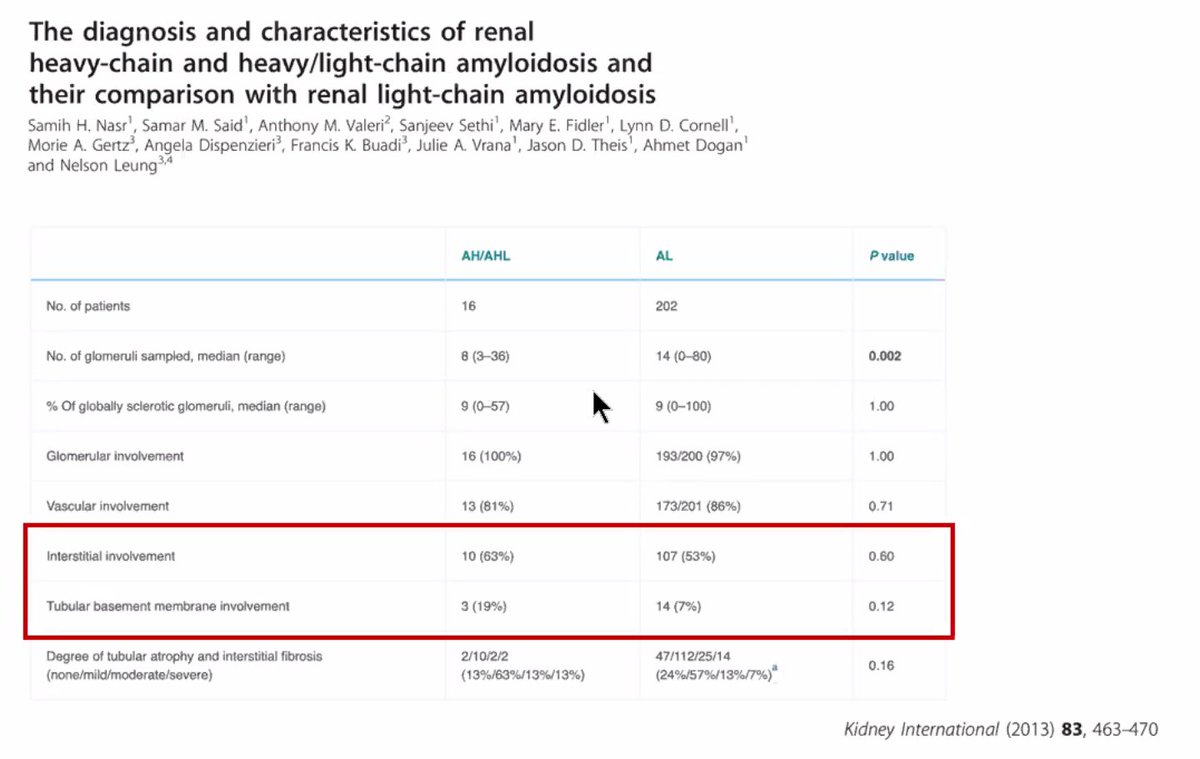
Distribution of amyloidosis by renal compartments:
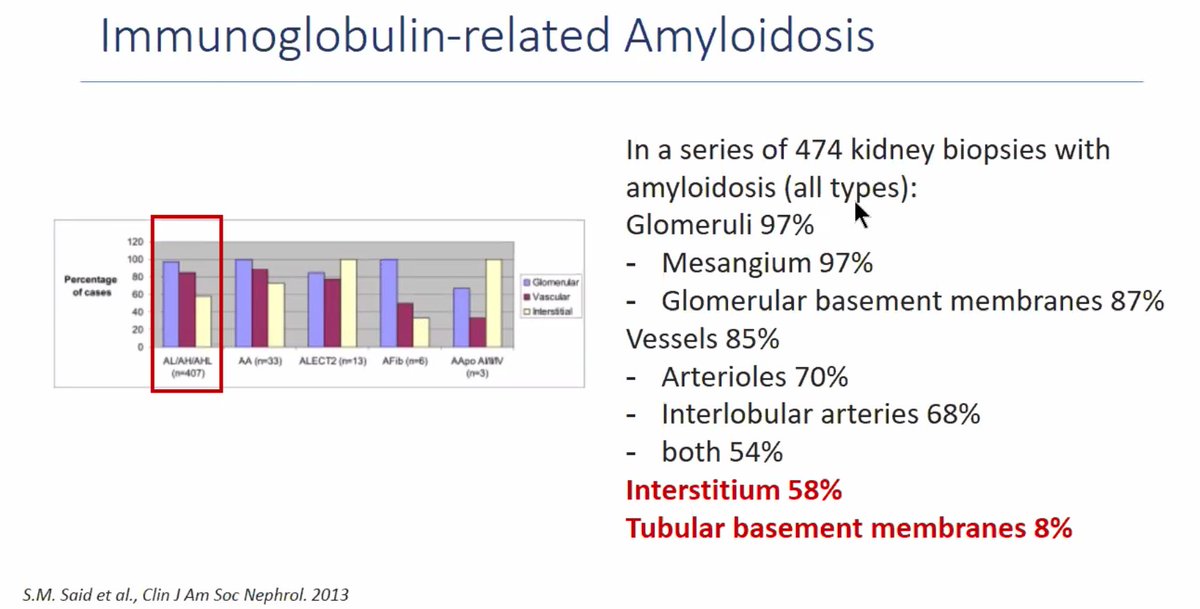
Characteristics of the monoclonal immunoglobulin make it amyloidogenic in AL or AHL amyloidosis.
Some conclusions:
@threadreaderapp unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh