1/
You’re starting a consult service block.
But this time is different.
-Maybe you don’t have a consult “team” to teach
-Maybe you want to showcase your specialty & recruit interested trainees
-Maybe you want to build ties to other service lines
What to do?
This week:
You’re starting a consult service block.
But this time is different.
-Maybe you don’t have a consult “team” to teach
-Maybe you want to showcase your specialty & recruit interested trainees
-Maybe you want to build ties to other service lines
What to do?
This week:
2/
@JenniferSpicer4 and I have spent the last few weeks exploring the "why", the "who", and the "when" of teaching the primary team in our role as consultants.
Now let's turn to the "what".
What repertoire of teaching scripts should we strive to develop as specialists?
@JenniferSpicer4 and I have spent the last few weeks exploring the "why", the "who", and the "when" of teaching the primary team in our role as consultants.
Now let's turn to the "what".
What repertoire of teaching scripts should we strive to develop as specialists?
3/
1⃣ Content knowledge
It's natural to gravitate toward teaching specialty-specific content - that's our expertise!
We've covered a lot of this territory in prior threads.
I'm going to highlight some of those pearls & point out specific strategies for teaching primary teams.
1⃣ Content knowledge
It's natural to gravitate toward teaching specialty-specific content - that's our expertise!
We've covered a lot of this territory in prior threads.
I'm going to highlight some of those pearls & point out specific strategies for teaching primary teams.
4/
Most of us think about teaching "content" to primary teams at the time we deliver recommendations.
To do so most effectively, it's worth revisiting the factors that determine "where" a learner is.
Those factors impact what content we can teach.
Most of us think about teaching "content" to primary teams at the time we deliver recommendations.
To do so most effectively, it's worth revisiting the factors that determine "where" a learner is.
Those factors impact what content we can teach.
https://twitter.com/VarunPhadke2/status/1605245928549629960?s=20
5/
Let’s start w/ teaching when delivering recs in-person.
Here, it makes most sense to use the consult “type” to guide your teaching:
📌 Differentiated problem ➡️ scripts
📌 Undifferentiated problem ➡️ schemas
📌 Management decision ➡️ risks/benefits
Let’s start w/ teaching when delivering recs in-person.
Here, it makes most sense to use the consult “type” to guide your teaching:
📌 Differentiated problem ➡️ scripts
📌 Undifferentiated problem ➡️ schemas
📌 Management decision ➡️ risks/benefits

6/
Obviously, there's a LOT that one could teach.
But I'm going to make a special plug for teaching schemas (a la @CPSolvers).
Schemas allow you to reinforce what the primary team has already done, add nuance, & build autonomy.
Effective schemas empower learners.
Obviously, there's a LOT that one could teach.
But I'm going to make a special plug for teaching schemas (a la @CPSolvers).
Schemas allow you to reinforce what the primary team has already done, add nuance, & build autonomy.
Effective schemas empower learners.
7/
In a previous thread, I shared strategies for building schemas for members of the consult team.
The same principles can also be discussed with primary teams.
But here are some additional concrete strategies that apply specifically to primary teams.
In a previous thread, I shared strategies for building schemas for members of the consult team.
The same principles can also be discussed with primary teams.
But here are some additional concrete strategies that apply specifically to primary teams.
https://twitter.com/VarunPhadke2/status/1623163962157150208?s=20

8/
I also believe it is our responsibility as consultants to teach WHY we recommend a certain diagnostic pathway or therapeutic option.
This means being transparent about factors influencing our decision-making.
Doing this in-person mitigates conflict.
I also believe it is our responsibility as consultants to teach WHY we recommend a certain diagnostic pathway or therapeutic option.
This means being transparent about factors influencing our decision-making.
Doing this in-person mitigates conflict.
https://twitter.com/VarunPhadke2/status/1615422036196659213?s=20
9/
Now let's hit ⏸️ & recognize that although many consider in-person delivery of recs to be the 🎯, that’s not reality.
More often than not, we are delivering recs by 📞.
On the phone, your limitations are:
⏲️ Time
🥱 Attention span
🫥 No visuals
Now let's hit ⏸️ & recognize that although many consider in-person delivery of recs to be the 🎯, that’s not reality.
More often than not, we are delivering recs by 📞.
On the phone, your limitations are:
⏲️ Time
🥱 Attention span
🫥 No visuals
https://twitter.com/VarunPhadke2/status/1605245918994960386?s=20
10/
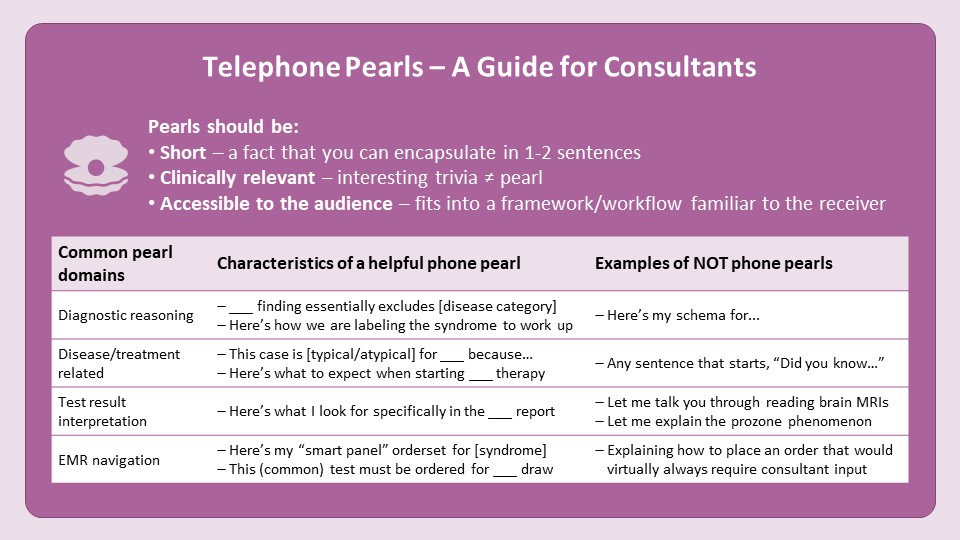
So, what CAN we teach on the phone?
The ideal telephone teaching point needs to be:
*⃣ Short
*⃣ Clinically relevant
*⃣ Accessible to the audience
In essence, it should be a clinical PEARL.
pubmed.ncbi.nlm.nih.gov/18821165/
So, what CAN we teach on the phone?
The ideal telephone teaching point needs to be:
*⃣ Short
*⃣ Clinically relevant
*⃣ Accessible to the audience
In essence, it should be a clinical PEARL.
pubmed.ncbi.nlm.nih.gov/18821165/
11/
2⃣ Processes
Now let’s move beyond scripts/schemas. We can also teach primary teams our processes – these are skills.
This often takes us beyond the "delivery of recs" encounter to other teaching contexts, such as:
🛌 Teaching at the bedside
🧑🤝🧑 Multidisciplinary teaching
2⃣ Processes
Now let’s move beyond scripts/schemas. We can also teach primary teams our processes – these are skills.
This often takes us beyond the "delivery of recs" encounter to other teaching contexts, such as:
🛌 Teaching at the bedside
🧑🤝🧑 Multidisciplinary teaching
12/
Last week @JenniferSpicer4 shared examples of what to teach primary teams at the bedside.
While this teaching often occurs on-the-fly, by actively reflecting on things we do often (read: subconsciously) we can generate scripts more intentionally.
Last week @JenniferSpicer4 shared examples of what to teach primary teams at the bedside.
While this teaching often occurs on-the-fly, by actively reflecting on things we do often (read: subconsciously) we can generate scripts more intentionally.
https://twitter.com/JenniferSpicer4/status/1633162204324196381?s=20

13/
@JenniferSpicer4 also described venues for us to teach through our interactions w/ other healthcare professionals.
In these settings, we can teach:
💬 WHAT questions to ask (in radiology, micro, etc)
⌚️ WHEN to ask them
🗣️ HOW to ask them (framing)
@JenniferSpicer4 also described venues for us to teach through our interactions w/ other healthcare professionals.
In these settings, we can teach:
💬 WHAT questions to ask (in radiology, micro, etc)
⌚️ WHEN to ask them
🗣️ HOW to ask them (framing)
https://twitter.com/JenniferSpicer4/status/1633162199622381568?s=20
14/
In this 🧵 I’ve focused on domains of teaching scripts targeting the primary team (the one requesting the consult).
But remember that we interact with many other learners in our work as consultants.
We can be intentional about teaching them too!
In this 🧵 I’ve focused on domains of teaching scripts targeting the primary team (the one requesting the consult).
But remember that we interact with many other learners in our work as consultants.
We can be intentional about teaching them too!
https://twitter.com/VarunPhadke2/status/1630620645749932048?s=20
15/
In summary:
📌 We can teach content knowledge or processes depending on the context
📌 Always identify "where" your learner is when teaching the primary team
📌 In-person teaching is best tailored to the consult “type”
📌 Telephone teaching should be limited to “pearls”
In summary:
📌 We can teach content knowledge or processes depending on the context
📌 Always identify "where" your learner is when teaching the primary team
📌 In-person teaching is best tailored to the consult “type”
📌 Telephone teaching should be limited to “pearls”

16/
Next week @JenniferSpicer4 will wrap up this series on #SubspecialtyTeaching with a “Summary” thread.
Remember to check out @MedEdTwagTeam & follow @YihanYangMD @GStetsonMD @ChrisDJacksonMD to keep up with all our threads!
Thanks for joining and see you next week!
Next week @JenniferSpicer4 will wrap up this series on #SubspecialtyTeaching with a “Summary” thread.
Remember to check out @MedEdTwagTeam & follow @YihanYangMD @GStetsonMD @ChrisDJacksonMD to keep up with all our threads!
Thanks for joining and see you next week!

• • •
Missing some Tweet in this thread? You can try to
force a refresh