(1/20) “PE Thrombectomy Tweetorial”
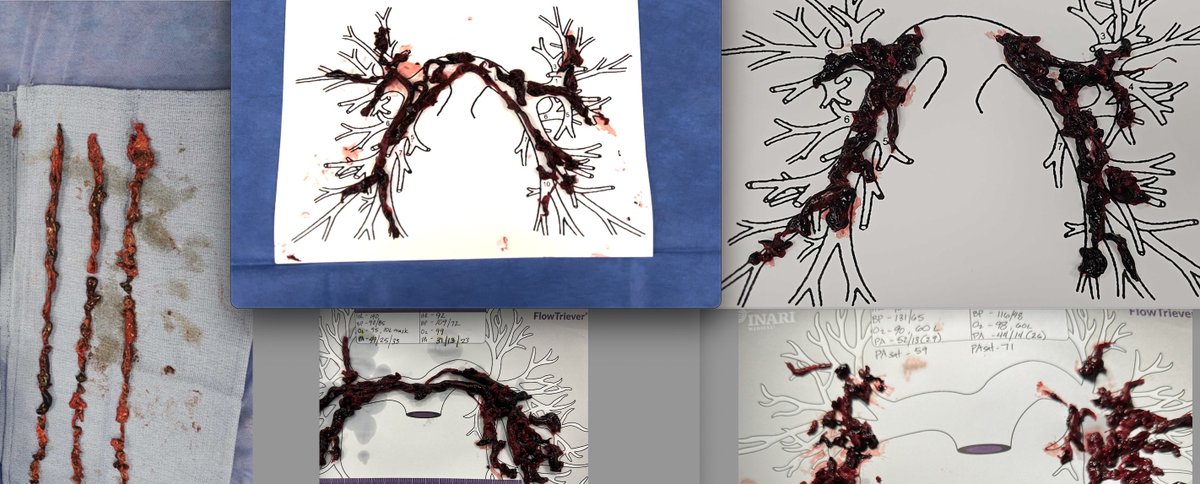
7 PE thrombectomy cases in the last few days @UABStructural #UABPERT. All patients got discharged 1-2 days post procedure. @MustafaAhmedMD @MouhamedAmr1 @Skmcelwee @Dr_AbuDaya @dprime45 @PhillipASmithMD @BaranAksutMD @DocEBROhimi @Dr_Almubarak
7 PE thrombectomy cases in the last few days @UABStructural #UABPERT. All patients got discharged 1-2 days post procedure. @MustafaAhmedMD @MouhamedAmr1 @Skmcelwee @Dr_AbuDaya @dprime45 @PhillipASmithMD @BaranAksutMD @DocEBROhimi @Dr_Almubarak

(2/20)
Preplanning:
•We activate the PERT team for any massive or submassive PE
•Multidisciplinary discussion for each case to decide on management
•It is critical to review the CT angiography, Echo images, lab values, and hemodynamics for each case.
Preplanning:
•We activate the PERT team for any massive or submassive PE
•Multidisciplinary discussion for each case to decide on management
•It is critical to review the CT angiography, Echo images, lab values, and hemodynamics for each case.

(3/20) Preparation of Triever 24F catheter:
-Dilator comes loaded in the catheter
-Flush the dilator and click it into place
-Side port comes turned on -> turn it off
-There is a one-way flush port, you twist the syringe on it and flush
-Keep the side port turned off
-Dilator comes loaded in the catheter
-Flush the dilator and click it into place
-Side port comes turned on -> turn it off
-There is a one-way flush port, you twist the syringe on it and flush
-Keep the side port turned off
(4/20) Preparation of Triever 20 F curved catheter:
-Take the dilator out and load it into the catheter and click it into place
-Turn the side port off
-Flush through the one-way flush port and the dilator as shown
-Take the dilator out and load it into the catheter and click it into place
-Turn the side port off
-Flush through the one-way flush port and the dilator as shown
(5/20) Preparation of FlowSaver – filter system:
- Take the purple cap out, attach the preloaded syringe to the one-way flush port and flush the filter, leave the syringe attached, and connect back to the filter as shown.
- Take the purple cap out, attach the preloaded syringe to the one-way flush port and flush the filter, leave the syringe attached, and connect back to the filter as shown.
(6/20) ECMO candidacy
-We assess the candidacy of ECMO for all high-risk patients (massive PE, submassive PE with hemodynamic instability)
-If high risk for decompensation: We also obtain left femoral arterial and vein accesses in case emergent ECMO cannulation is needed
-We assess the candidacy of ECMO for all high-risk patients (massive PE, submassive PE with hemodynamic instability)
-If high risk for decompensation: We also obtain left femoral arterial and vein accesses in case emergent ECMO cannulation is needed
(7/20) Mechanical thrombectomy steps:
-We obtain right femoral vein access, we put Perclose and then we place 24F dry seal after serial dilation. twitter.com/i/web/status/1…
-We obtain right femoral vein access, we put Perclose and then we place 24F dry seal after serial dilation. twitter.com/i/web/status/1…
(8/20)
We perform the RHC for pre-intervention hemodynamics, and then we advance a multipurpose catheter and wholey wire to find a good size branch in the right PA.
We perform the RHC for pre-intervention hemodynamics, and then we advance a multipurpose catheter and wholey wire to find a good size branch in the right PA.

(9/20)
At UAB, we connect a venous return tubing to the side port of the dry seal sheath. This tubing is used to return the filtered blood back to the patient.
At UAB, we connect a venous return tubing to the side port of the dry seal sheath. This tubing is used to return the filtered blood back to the patient.

(10/20)
Next, we then advance an Amplatz stiff wire into the pulmonary artery.
Next, we then advance an Amplatz stiff wire into the pulmonary artery.

(11/20)
We advance the 24F catheter over the stiff wire into the main PA then remove the dilator keeping the wire in place.
We advance the 24F catheter over the stiff wire into the main PA then remove the dilator keeping the wire in place.
(12/20)
-We then perform pulmonary angiogram using the 24F Triever catheter
-When performing pulmonary angiogram: we give 15cc contrast into the side port of the Triever 24F catheter and use 30cc normal saline as a chaser to get a good angiogram without giving a lot of contrast
-We then perform pulmonary angiogram using the 24F Triever catheter
-When performing pulmonary angiogram: we give 15cc contrast into the side port of the Triever 24F catheter and use 30cc normal saline as a chaser to get a good angiogram without giving a lot of contrast
(13/20)
-We then position the 24F catheter tip near the right PA clot and start suctioning
-While suctioning, we slowly walk the catheter back to facilitate clot suctioning
-We then position the 24F catheter tip near the right PA clot and start suctioning
-While suctioning, we slowly walk the catheter back to facilitate clot suctioning
(14/20)
After suctioning, we use this FlowSaver filter system to isolate the clots and return the rest of the blood back using the venous return tubing
After suctioning, we use this FlowSaver filter system to isolate the clots and return the rest of the blood back using the venous return tubing
(15/20)
- After finishing the thrombectomy of the right PA, we take the Triever 24F catheter out. We then move to the left PA using the Tiger catheter and wholey wire
- We perform the same steps doing thrombectomy of the left PA
- After finishing the thrombectomy of the right PA, we take the Triever 24F catheter out. We then move to the left PA using the Tiger catheter and wholey wire
- We perform the same steps doing thrombectomy of the left PA
(16/20)
Tip: If we need to use the 20F curved catheter for smaller branches or segmental PE, we can insert it through the 24F catheter as shown in this picture.
Tip: If we need to use the 20F curved catheter for smaller branches or segmental PE, we can insert it through the 24F catheter as shown in this picture.

(17/20)
We deploy the previously placed perclose achieving complete hemostasis.
We deploy the previously placed perclose achieving complete hemostasis.

(18/20)
During the case, the fellow can be assigned to different roles based on the complexity of the case and the level of training.
During the case, the fellow can be assigned to different roles based on the complexity of the case and the level of training.

(19/20)
- During the procedure, our ACT goal is >250
- Usually, our patients get discharged in 1-2 days post-procedure
- All our PE patients get follow-up with a multidisciplinary post PE network involving cardiology, pulmonary, and hematology clinics
- During the procedure, our ACT goal is >250
- Usually, our patients get discharged in 1-2 days post-procedure
- All our PE patients get follow-up with a multidisciplinary post PE network involving cardiology, pulmonary, and hematology clinics
(20/20)
We use different technologies at UAB to manage PE patients including IV anticoagulation, catheter-directed thrombolytic therapy, and mechanical thrombectomy.
We use different technologies at UAB to manage PE patients including IV anticoagulation, catheter-directed thrombolytic therapy, and mechanical thrombectomy.
@KyleEudaileyMD @pannvar @RootGal210
@AlaMohsen87 @TEWatts3
@ShanePrejeanMD @GarimaAroraMD @nnishank52 @_C9_H13_NO3
@MarkLaw80307275 @Katie_Evatt @AshleyReed_RT @AlainBouchardmd @HassanAlkhawam @_Calder_1017_ @AgastyaBelur @RuchitShahMD @NicoleLohrMD @UABCardiology @UABCVI
@AlaMohsen87 @TEWatts3
@ShanePrejeanMD @GarimaAroraMD @nnishank52 @_C9_H13_NO3
@MarkLaw80307275 @Katie_Evatt @AshleyReed_RT @AlainBouchardmd @HassanAlkhawam @_Calder_1017_ @AgastyaBelur @RuchitShahMD @NicoleLohrMD @UABCardiology @UABCVI
@jmmoody5973 @HadyLichaaMD @DrAlsubei @ChipSosa @LchaconMD @RaeganWhite6 @Nidhi_Madan9 @KateKearney4 @DrJayMohan
• • •
Missing some Tweet in this thread? You can try to
force a refresh