
My notifications have been exploding over this paper, so some words on it:
reader.elsevier.com/reader/sd/pii/…
Firstly, there's a big fallacy I'm seeing committed in some people's interpretations of the paper:
reader.elsevier.com/reader/sd/pii/…
Firstly, there's a big fallacy I'm seeing committed in some people's interpretations of the paper:
People are again fixating on mechanisms over epidemiology. Hybrid immunity to SARS-CoV-2 gives superior protection to every other form of immunity. This is abundantly clear in literally every epidemiological study looking at it. Note that this should not justify...
trying to get infected by SARS-CoV-2 as a path to immunity, especially sans vaccination, because that's ridiculously dangerous. Having said that, I don't really agree with (aspects of) the paper's interpretation of its data.
The part that's causing all of the ruckus is the claim that SARS-CoV-2 infection results in CD8 T cell functional impairment. I really don't find this to be well supported by the data in this paper. Firstly, the vaccine contains only spike protein.
It's really amazing that the vaccine does an obviously superior job at inducing T cell responses against the spike protein and it's noteworthy that the response is concentrated in TCM cells as this supports durability of the T cell response. 
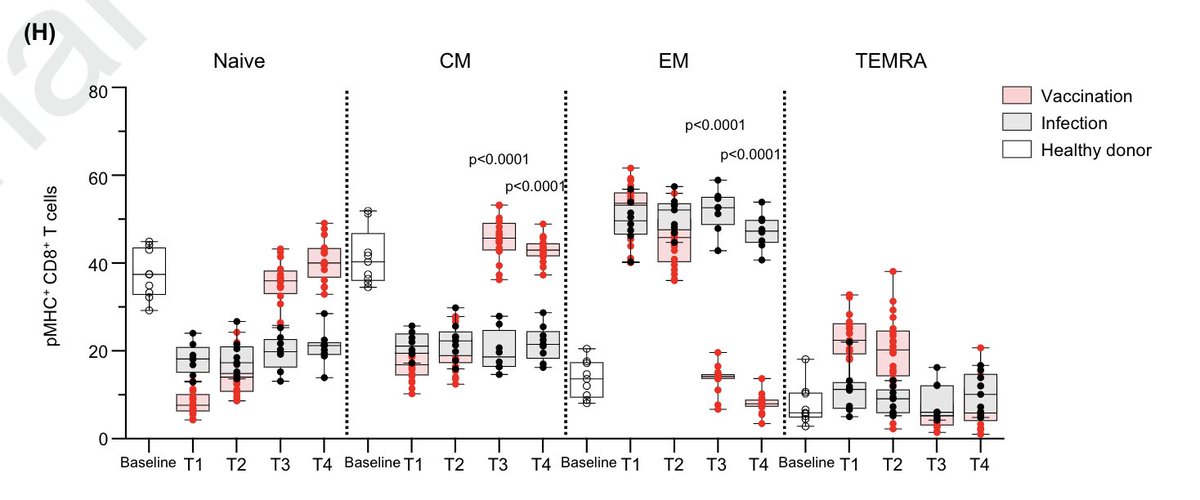
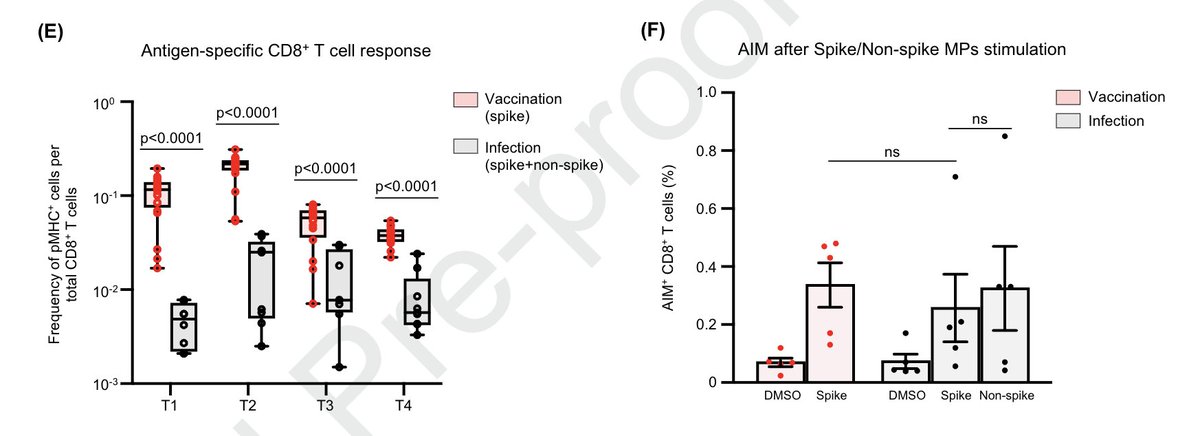
However, there's no obvious deficit in the ability of T cells from COVID-19 convalescents to respond to SARS-CoV-2 epitopes here. CD8 T cell responses induced by infection will target epitopes beyond spike. The AIM assay shows pretty comparable results for vaccine vs infection.
Then comes the hybrid immunity bit: what happens to T cells when people who recovered get the vaccine? Here we see that the total response (not though this isn't an AIM assay) is smaller compared with naive patients. So- is that it? COVID wrecked their CD8 T cells?
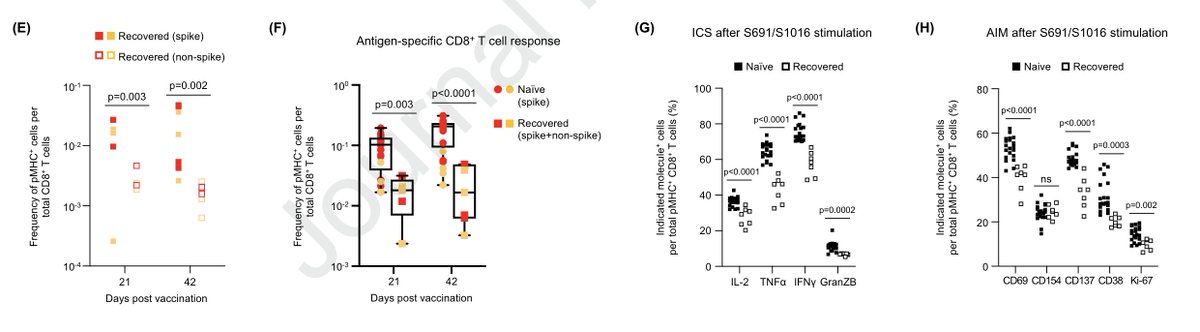
That seems like quite a stretch. In essence, their immune system is more extensively primed against any SARS-CoV-2 antigens compared with someone getting the vaccine for the first time without a history of infection. It seems far more likely to me, especially given...
that CD8 T cell responses peak later with mRNA vaccines than CD4 T cell responses, that their extensively primed immune system is able to deal with the vaccine more quickly and doesn't get as much stimulation to its CD8 T cell compartment compared with those who aren't infected.
In support of this, there is the finding that the second dose of vaccine didn't do much of anything for CD8 T cell responses, which we now know from other work is probably attributable to dosing interval:
cell.com/cell/pdf/S0092…
cell.com/cell/pdf/S0092…
Additionally, because these are peripheral T cells (taken by blood draw), they might not capture all that is happening, particularly when looking at the mucosae.
Indeed, those who are infected and subsequently receive vaccines develop T cells that home to the mucosae:
biorxiv.org/content/10.110…
If we are to take the worst-case scenario that this is SARS-CoV-2 doing bad things to CD8 T cells, this basically underscores the importance...
biorxiv.org/content/10.110…
If we are to take the worst-case scenario that this is SARS-CoV-2 doing bad things to CD8 T cells, this basically underscores the importance...
of getting vaccinated before you have a chance to become infected. But, truthfully, I'm not convinced the presented data show actual CD8 dysfunction and the litany of clinical data on hybrid immunity argue against it.
• • •
Missing some Tweet in this thread? You can try to
force a refresh







