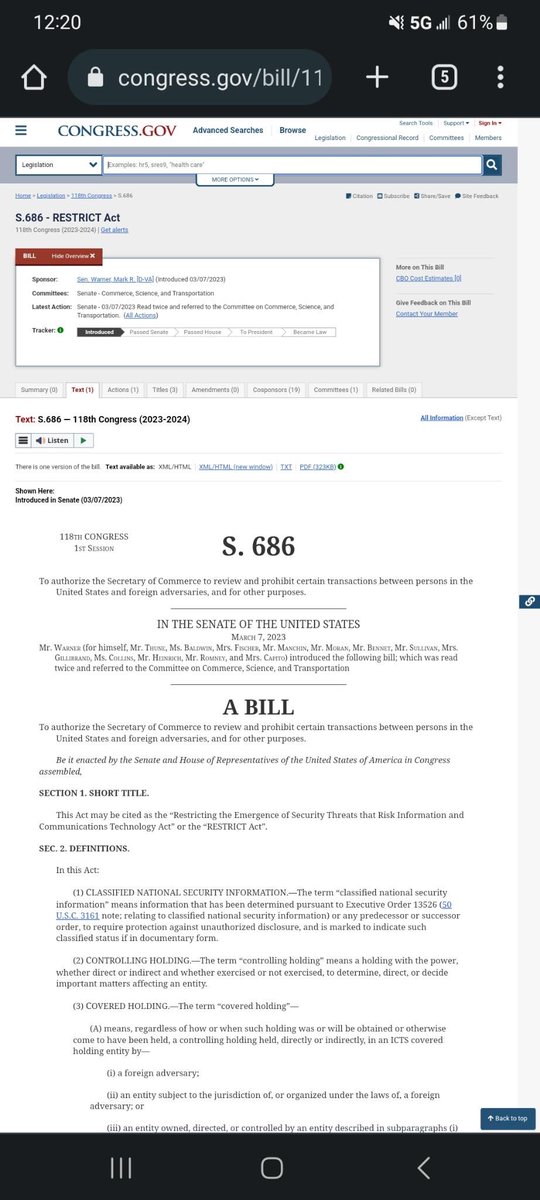
Everyone needs to hear about the RESTRICT Act (S. 686). This bill is also currently known as the "Tik Tok ban" by many. But, it looks as though we were all deceived again. The Tik Tok ban is nothing but a distraction while they try to push the RESTRICT Act into law. 


If this bill gets passed, we lose almost all privacy we have. The attached screenshots highlight only a few of my concerns with this bill;
"Any software, hardware, or any other product or service integral to the telecommunications products and services" with over 1,000,000
"Any software, hardware, or any other product or service integral to the telecommunications products and services" with over 1,000,000
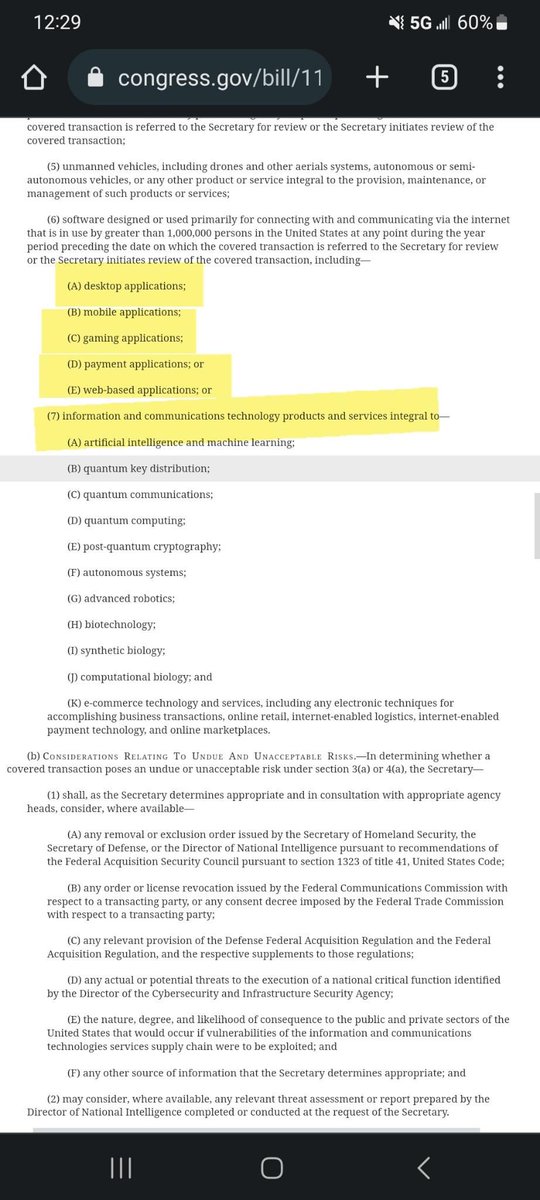
users would now be at the governments disposal to review, prosecute, and take possession of. They can "review" any and all of your personal information without even notifying you that they are doing so. They can ban any game, application, or thing they deem fit


if it "poses a risk".
The RESTRICT Act (S. 686) would allow the government to access all of the data on your video devices if it is a service that uses over 1,000,000 people, THIS INCLUDES SERVICES LIKE RING DOORBELL/INHOME SECURITY CAMERAS and so much more.
The RESTRICT Act (S. 686) would allow the government to access all of the data on your video devices if it is a service that uses over 1,000,000 people, THIS INCLUDES SERVICES LIKE RING DOORBELL/INHOME SECURITY CAMERAS and so much more.
A VPN won't help you get around this either, if caught using a privacy device such as a VPN, you will face up to 20 years in prison AND/OR up to $1,000,000 in fines.
We NEED to bring attention to this and tell our elected officials that we do NOT support the RESTRICT Act.
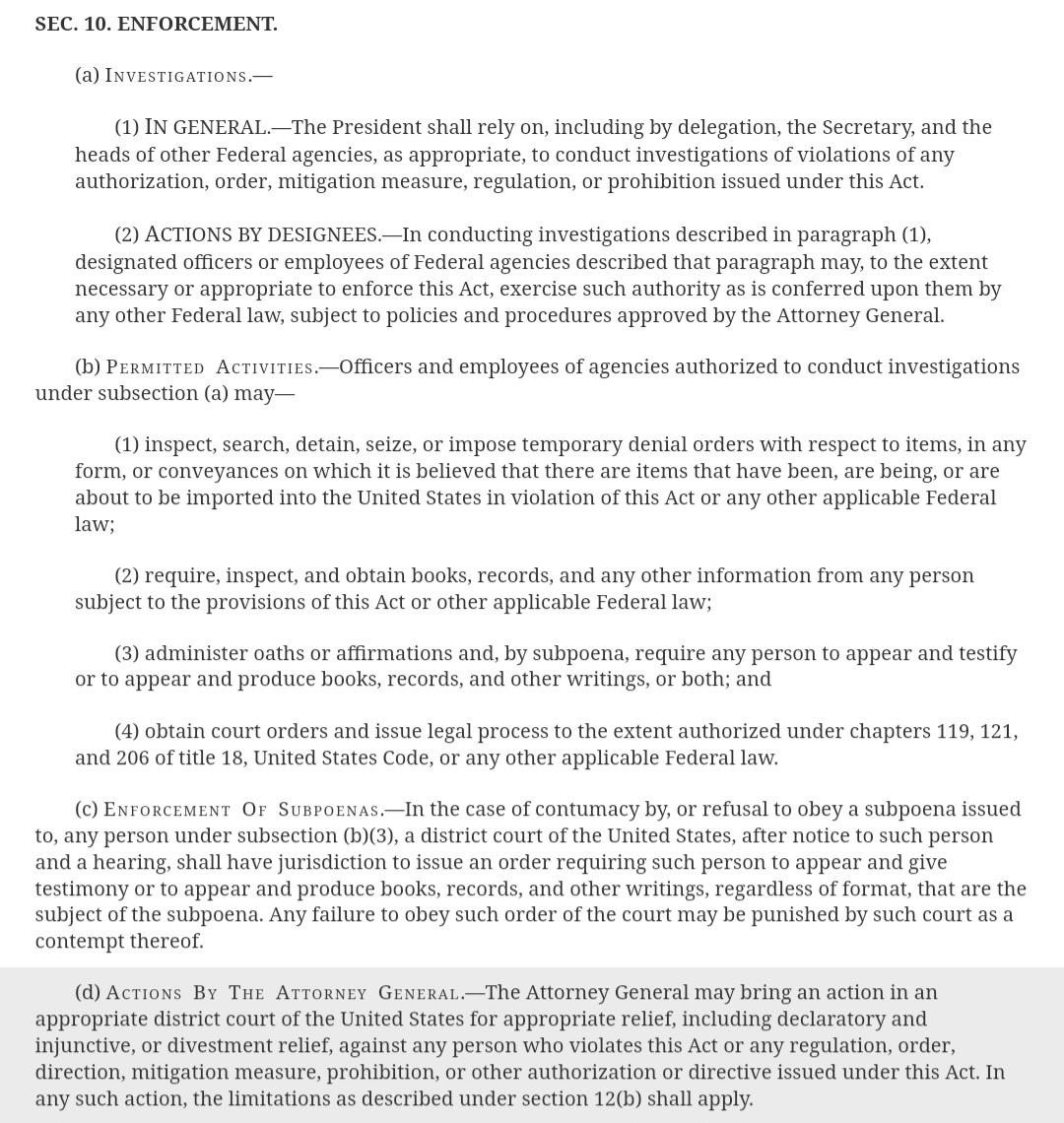
We NEED to bring attention to this and tell our elected officials that we do NOT support the RESTRICT Act.
Our thoughts, speech, ideas, identity and bodies are the target.
https://twitter.com/Plandemic3Movie/status/1639727275259174913
Video explaining in case you can’t read-
Part 2
• • •
Missing some Tweet in this thread? You can try to
force a refresh