Two groups representing LGBTQ+ medical professionals (@GLADDUK and @prism_surgery) submitted a letter of complaint to the prestigious British Medical Journal (@bmj_latest). 


The BMJ’s crime: pointing out problems in the “gender affirming care is science-based” narrative. GAC is consensus-based (that is, if you ignore doctors, medical groups, and European health authorities who disagree), but not evidence-based.
bmj.com/content/380/bm…
bmj.com/content/380/bm…
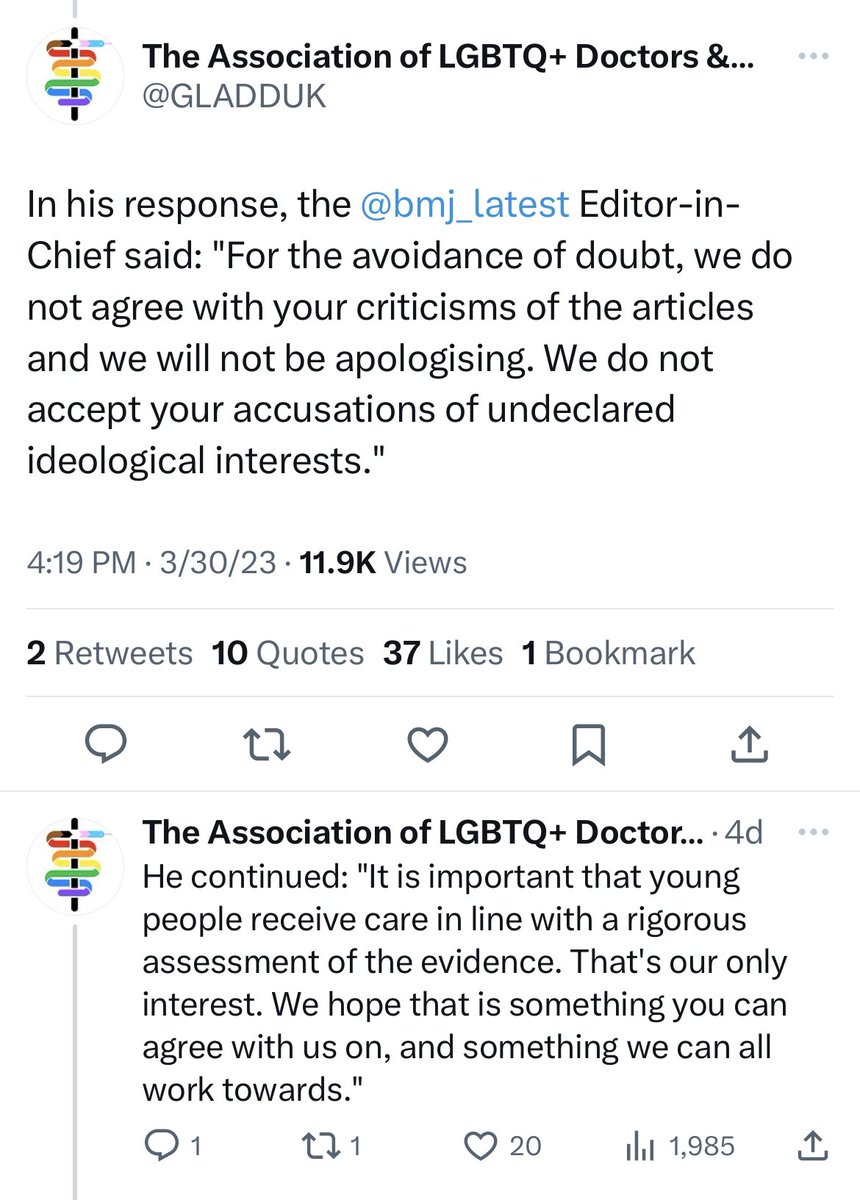
Since “the science is settled” on this issue and any questioning of that science is clear evidence of bigotry, the letter demanded an apology.
The two groups also demanded that the BMJ disclose whether the author or the editor harbor “gender critical” beliefs (read: beliefs that question the activist-approved narrative on pediatric gender medicine).
“Gender critical” beliefs, you see, are strictly verboten and those who adhere to them must confess and atone.
BMJ’s editor in chief politely declined the requests, telling the two orgs to fu… I mean, to rediscover their commitment to the scientific process.
Let’s hope American medical journals get inspired.
Let’s hope American medical journals get inspired.
• • •
Missing some Tweet in this thread? You can try to
force a refresh