
Lab guy from Yale up next Joe El Khoury He is on YouTube. Episode 1 was on pseudohyponatemia
209 subscribers. Clinical Chemistry with Joe El-Khoury
209 subscribers. Clinical Chemistry with Joe El-Khoury

Despite calling it “laboratory error”, a lot of the problem happens long before the sample gets to the lab. #NKFClinicals
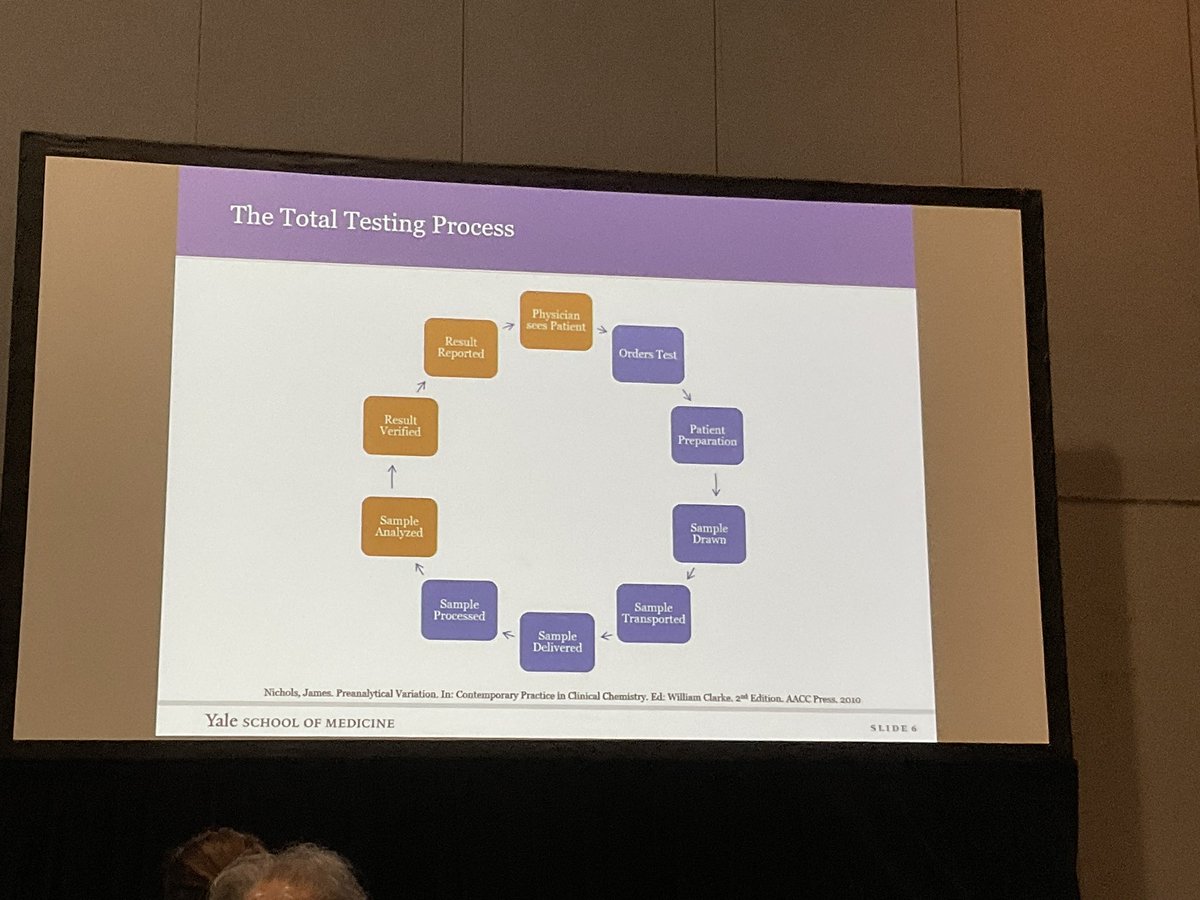
75% of errors happen before sample gets to the lab! #NKFClinicals
It is almost never an analytical issue. Because these guys are careful.
It is almost never an analytical issue. Because these guys are careful.

Case 1/6 K was 6 and normal in ER, this happens every January. The outpatient winter K is too high. He was symptomatic. Also occurs with sister.
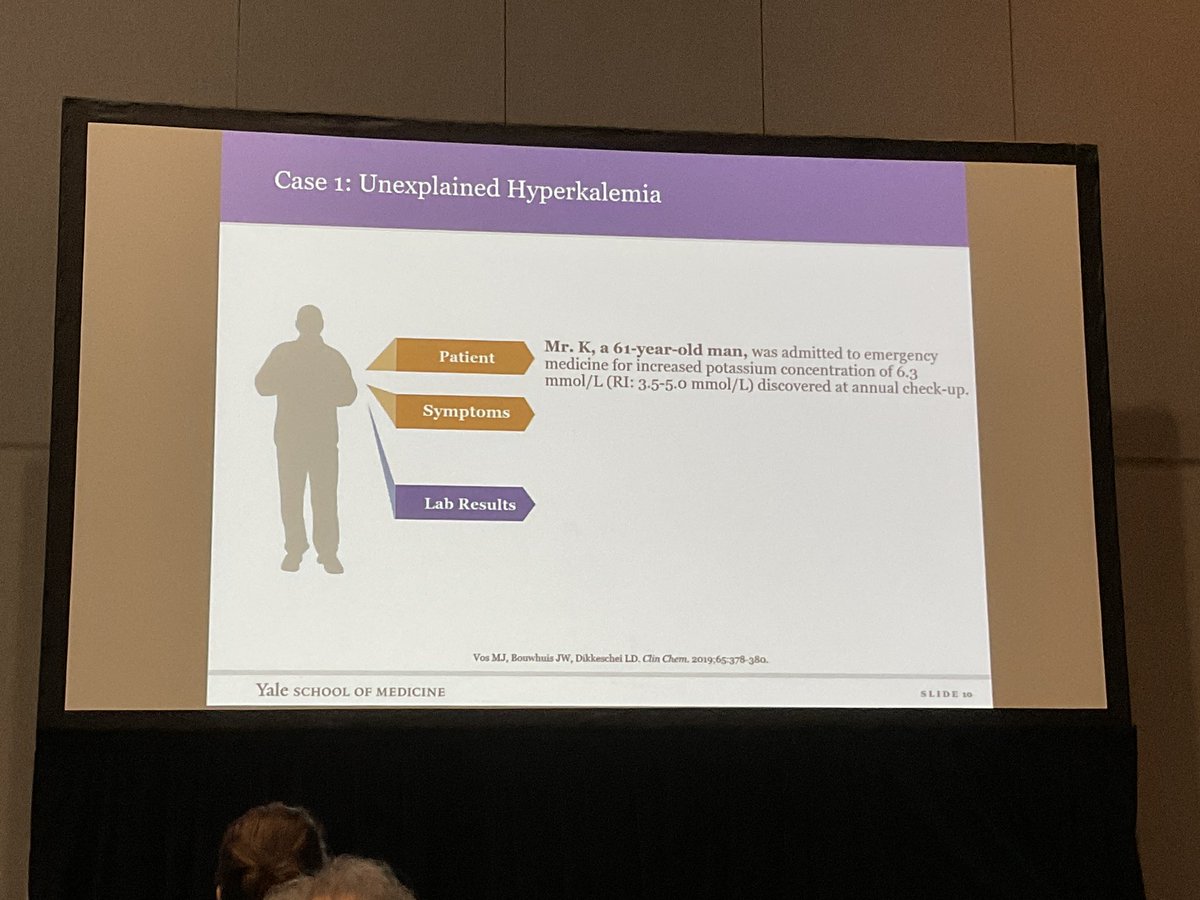
Familial Pseudohyperkalemia, they have fast leak in response to cooling and time.

If you spin the sample first to separate the cells from the plasma.

Case 2/6
Unexplained low CO2 in an infant
History of diarrhea
First sample 11 2 hours later it was 18.
The small ample in a big tube allows CO2 to escape resulting in artifact.
Unexplained low CO2 in an infant
History of diarrhea
First sample 11 2 hours later it was 18.
The small ample in a big tube allows CO2 to escape resulting in artifact.

Case 3
Elevations in lactate of 10 after surgery
On antibiotics.
Not concordat with clinical picture
Routine labs and ABG
3 days and 8 doctors to figure out they were drawing the labs downstream from an LR infusion 🤦🏼♂️ #NKFClinicals
Elevations in lactate of 10 after surgery
On antibiotics.
Not concordat with clinical picture
Routine labs and ABG
3 days and 8 doctors to figure out they were drawing the labs downstream from an LR infusion 🤦🏼♂️ #NKFClinicals



• • •
Missing some Tweet in this thread? You can try to
force a refresh















