
Day 3/Lecture 1: CKD
1. Cr and cystatin C: Cr has a diet source, cystat C does not (nor muscular influence). Musc young pt w/o RF and neg UA with an inc Cr has just that, not AKI!
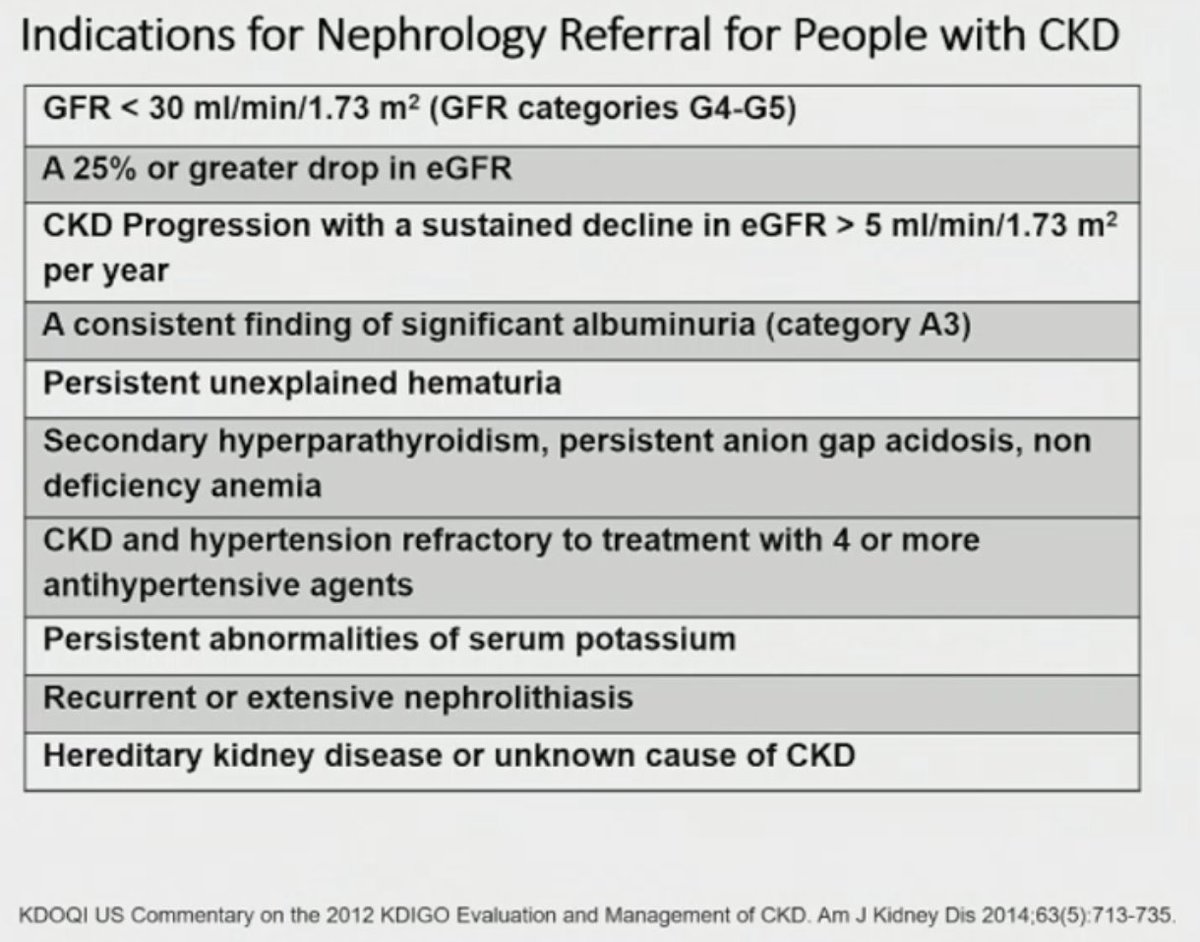
2. Indications for Nephrology Referral in patient's with CKD (see photo). #IM2023 @ACPIMPhysicians
1. Cr and cystatin C: Cr has a diet source, cystat C does not (nor muscular influence). Musc young pt w/o RF and neg UA with an inc Cr has just that, not AKI!
2. Indications for Nephrology Referral in patient's with CKD (see photo). #IM2023 @ACPIMPhysicians



4. SGLT2i + Finerinone (non-steroid MRA) attenuates CKD progress and HF hospitalization (not Semaglutide except w/CAD pts) even w/o hx of DM. + effect after max RASi on board.
5. Tx pts w/ DM+CKD with GFR > or = 30 cc/min w/ SGLT2i (Empa, Dapa, Canag).
#IM2023 @ACPIMPhysicians
5. Tx pts w/ DM+CKD with GFR > or = 30 cc/min w/ SGLT2i (Empa, Dapa, Canag).
#IM2023 @ACPIMPhysicians

6. SGLT2i not rec in DM1 pts (risk of DKA) and ADPCKD
7. Spiro/eplerenone with more data in HFrEF, Finerenone with more data in CKD.
8. Q of which to start first - SGLT2i or MRA, still remains.
9. Per KDIGO, sCr increase of 0.3 mg/dL in 48h = AKI.
#IM2023 @ACPIMPhysicians
7. Spiro/eplerenone with more data in HFrEF, Finerenone with more data in CKD.
8. Q of which to start first - SGLT2i or MRA, still remains.
9. Per KDIGO, sCr increase of 0.3 mg/dL in 48h = AKI.
#IM2023 @ACPIMPhysicians
10. Lower incidence of CA-AKI with routinely hypo- or iso-osmolar iodinated contrast modalities (min vol). Hydrate patients with CKD4 or worse with NS 3 cc/kg/h before and after such studies including cor angio.
#IM2023 @ACPIMPhysicians
#IM2023 @ACPIMPhysicians

11. With Group 2 Gad-based contrast media, harms of delaying or witholding GBCM for an MRI in a patient with AKI or eGFR<30 is likely to outweigh risk in most clinical situations.
#IM2023 @ACPIMPhysicians
#IM2023 @ACPIMPhysicians

12. Note: When initiating SGLT2i/MRA expect <30% rise in serum Cr and/or 30% drop d/t hemodynamic modulation. Consider dropping diuretic dosages in CKD patients.
13. Maximize RASi in patients with HTN and albuminuria.
14. Do we add finerenone after RASi or SGLT2i? Trial underway.
13. Maximize RASi in patients with HTN and albuminuria.
14. Do we add finerenone after RASi or SGLT2i? Trial underway.
@ACPIMPhysicians Saving for cystatin C content: journals.lww.com/kidney360/page…
• • •
Missing some Tweet in this thread? You can try to
force a refresh













