
Midmorning #VTA23 session starting - lots of short talks so expect quick changes in topic! #critcare #FOAMcc
PARDIE stands for Pediatric ARDS Incidence and Epidemiology study. This study is one of the results of the PALISI Conference Group.
doi.org/10.1016/S2213-…
#VTA23
doi.org/10.1016/S2213-…
#VTA23
The PALISI group looked at which oxygenation measurements may be used.
Options included:
PF ratio
SF ratio
OI
OSI
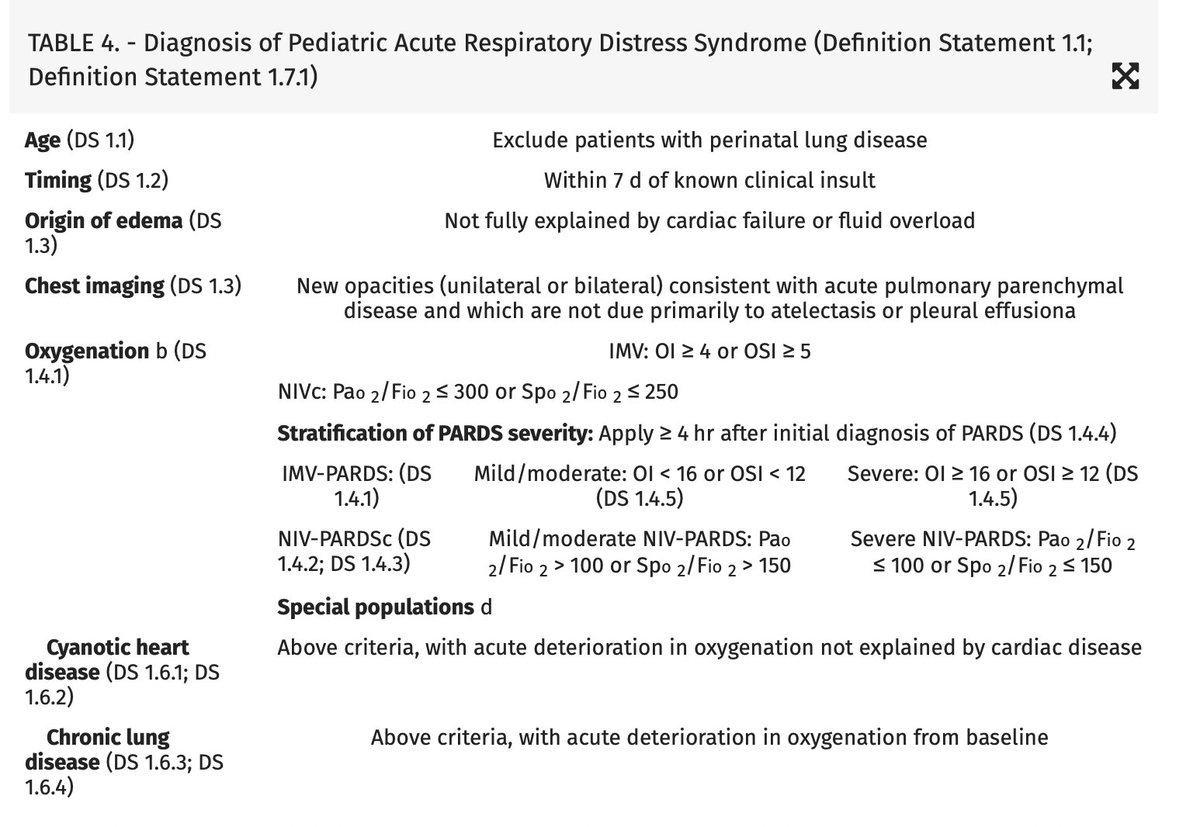
They also defined Paediatric ARDS, in 2015 and then again this year in 2023.
doi.org/10.1097/PCC.00…
doi.org/10.1097/PCC.00…
#VTA23
Options included:
PF ratio
SF ratio
OI
OSI
They also defined Paediatric ARDS, in 2015 and then again this year in 2023.
doi.org/10.1097/PCC.00…
doi.org/10.1097/PCC.00…
#VTA23
PARDIE looked at 145 PICUs worldwide, 23215 patients. 12270 were on mechanical ventilation.
744 new cases of PARDS were identified, 704 of which had complete data. It was a massive effort in a difficult to study population. #VTA23
744 new cases of PARDS were identified, 704 of which had complete data. It was a massive effort in a difficult to study population. #VTA23
PARDIE informed the new PARDS definition by PALISI - PALICC-2.
11 new sections
doi.org/10.1097/PCC.00…
#VTA23
11 new sections
doi.org/10.1097/PCC.00…
#VTA23
PARDIE take home messages:
PARDS affects 3% of PICU patients. Mortality is 30%. PALICC criteria are more sensitive than Berlin.
PALICC use of OI and OSI is a better predictor of mortality than PF and SF ratios.
However - HFOV, iNO and ECMO were not studied
#VTA23
PARDS affects 3% of PICU patients. Mortality is 30%. PALICC criteria are more sensitive than Berlin.
PALICC use of OI and OSI is a better predictor of mortality than PF and SF ratios.
However - HFOV, iNO and ECMO were not studied
#VTA23
• • •
Missing some Tweet in this thread? You can try to
force a refresh



