
1/28
You are the resident on CICU. A patient arrives with an intra-aortic balloon pump (IABP). What is it? How does it work? How do you troubleshoot?
It's ⏰ for a @CardioNerds tweetorial!
AKA things I've gotten wrong on rounds so you don't have to.
First up: the basics
You are the resident on CICU. A patient arrives with an intra-aortic balloon pump (IABP). What is it? How does it work? How do you troubleshoot?
It's ⏰ for a @CardioNerds tweetorial!
AKA things I've gotten wrong on rounds so you don't have to.
First up: the basics
2/28
What is an IABP?
- Counterpulsation device that supports the heart
- Catheter with helium-filled balloon at one end
- Balloon placed into descending aorta--the distal tip (when placed via femoral access) is just inferior to L subclavian artery, around the level of the carina
What is an IABP?
- Counterpulsation device that supports the heart
- Catheter with helium-filled balloon at one end
- Balloon placed into descending aorta--the distal tip (when placed via femoral access) is just inferior to L subclavian artery, around the level of the carina
3/28
How are IABPs placed?
Can be placed via a femoral or upper extremity approach (via subclavian, axillary, or brachial arteries).
A note re: lingo: the upper extremity approach is often referred to as an "axillary" approach even if it is not placed via the axillary artery.
How are IABPs placed?
Can be placed via a femoral or upper extremity approach (via subclavian, axillary, or brachial arteries).
A note re: lingo: the upper extremity approach is often referred to as an "axillary" approach even if it is not placed via the axillary artery.
4/28
How are they positioned?
One end in prox descending aorta just distal to L subclavian artery (~2cm above the carina on CXR)
Other end is in the mid-abdominal aorta
Note: proximal vs distal lingo depends on axillary vs femoral placement. Figure below = femoral placement.
How are they positioned?
One end in prox descending aorta just distal to L subclavian artery (~2cm above the carina on CXR)
Other end is in the mid-abdominal aorta
Note: proximal vs distal lingo depends on axillary vs femoral placement. Figure below = femoral placement.


5/28
Why is positioning important?
- Too high: occludes subclavian arteries
- Too low: occludes renal arteries
How can you determine positioning?
- CXR! Radio-opaque tip at the distal end.
- Note: this balloon is placed via femoral artery
Why is positioning important?
- Too high: occludes subclavian arteries
- Too low: occludes renal arteries
How can you determine positioning?
- CXR! Radio-opaque tip at the distal end.
- Note: this balloon is placed via femoral artery

6/28
Some (not all) reasons that you may see a 🎈:
Cardiogenic shock (AMI & HF)
Complex PCI
Refractory angina awaiting revasc.
Some (not all) reasons a 🎈may be inappropriate:
Aortic regurg
Aortic dissection, aneurysm
Aortic grafts/stents
Significant PVD
Sepsis
Bleeding
Some (not all) reasons that you may see a 🎈:
Cardiogenic shock (AMI & HF)
Complex PCI
Refractory angina awaiting revasc.
Some (not all) reasons a 🎈may be inappropriate:
Aortic regurg
Aortic dissection, aneurysm
Aortic grafts/stents
Significant PVD
Sepsis
Bleeding
7/28
How does an IABP work?
Balloon inflates and deflates with cardiac cycle
INFLATES in DIASTOLE and DEFLATES in SYSTOLE--counterpulsation!
Can set the IABP to do this every cycle (1:1), every other (1:2), or every two (1:3)
(NOTE: assuming nl compliance)
How does an IABP work?
Balloon inflates and deflates with cardiac cycle
INFLATES in DIASTOLE and DEFLATES in SYSTOLE--counterpulsation!
Can set the IABP to do this every cycle (1:1), every other (1:2), or every two (1:3)
(NOTE: assuming nl compliance)
8/28
First: inflation at the beginning of diastole
What happens in diastole in a normal heart?
🎈LV is relaxed & coronary arteries fill
First: inflation at the beginning of diastole
What happens in diastole in a normal heart?
🎈LV is relaxed & coronary arteries fill
9/28
What does IABP inflation do?
🎈Increases the diastolic pressure in the aorta (because it's inflated!)
🎈Inflates at the beginning of diastole ➡️ increase in coronary perfusion pressure. This increase in pressure improves myocardial O2 supply.
What does IABP inflation do?
🎈Increases the diastolic pressure in the aorta (because it's inflated!)
🎈Inflates at the beginning of diastole ➡️ increase in coronary perfusion pressure. This increase in pressure improves myocardial O2 supply.
10/28
Second: IABP deflation at the onset of systole
What happens in a normal heart?
🎈LV pressure > aortic pressure --> AV open --> start of ventricular ejection
🎈 As blood leaves LV & enters the aorta, get ⬆️ in systemic pressure & ⬇️ in LV pressure due to changes in volume
Second: IABP deflation at the onset of systole
What happens in a normal heart?
🎈LV pressure > aortic pressure --> AV open --> start of ventricular ejection
🎈 As blood leaves LV & enters the aorta, get ⬆️ in systemic pressure & ⬇️ in LV pressure due to changes in volume
11/28
What does IABP deflation do?
🎈 Deflation decreases aortic EDP, so the LV is working against less resistance & and there is less systolic wall tension (decreased LV afterload)
🎈 Small vacuum effect in proximal aorta, which decreases LV afterload
What does IABP deflation do?
🎈 Deflation decreases aortic EDP, so the LV is working against less resistance & and there is less systolic wall tension (decreased LV afterload)
🎈 Small vacuum effect in proximal aorta, which decreases LV afterload
12/28
Note that it decreases afterload without necessarily changing the MAP due to the increase in diastolic pressure!
Why is this good?
🎈Decreased myocardial oxygen demand
🎈Decreased LV afterload, increased LV stroke volume & cardiac output
Note that it decreases afterload without necessarily changing the MAP due to the increase in diastolic pressure!
Why is this good?
🎈Decreased myocardial oxygen demand
🎈Decreased LV afterload, increased LV stroke volume & cardiac output
13/28
Equations I find helpful to think through this:
CPP = DBP - LVEDP
The IABP increases DBP and decreases LVEDP --> increased CPP
Coronary blood flow (CBF) = CPP/coronary vascular resistance
So, assuming constant CVR, CPP is directly proportional to CBF
Equations I find helpful to think through this:
CPP = DBP - LVEDP
The IABP increases DBP and decreases LVEDP --> increased CPP
Coronary blood flow (CBF) = CPP/coronary vascular resistance
So, assuming constant CVR, CPP is directly proportional to CBF
14/28
Of note, the increase in CPP does not always translate to increased CBF.
Though we are focusing on basics, it's important to note that when coronary autoregulation works properly (when CVR changes to maintain a constant CBF), CPP changes may not translate to CBF changes
Of note, the increase in CPP does not always translate to increased CBF.
Though we are focusing on basics, it's important to note that when coronary autoregulation works properly (when CVR changes to maintain a constant CBF), CPP changes may not translate to CBF changes
15/28
Quick recap, part 1:
Inflation at onset of diastole
-- Inflation improves O2 supply via increased CPP
Deflation just before systole
-- Deflation reduces LV afterload which decreases O2 demand, increases LV stroke volume and cardiac output
Quick recap, part 1:
Inflation at onset of diastole
-- Inflation improves O2 supply via increased CPP
Deflation just before systole
-- Deflation reduces LV afterload which decreases O2 demand, increases LV stroke volume and cardiac output
16/28
Quick recap, part 2:
--Inflation pushes 🩸 into coronaries & raises systemic diastolic pressure (this is called diastolic augmentation)
--Deflation decreases aortic pressure & lowers systolic wall tension (afterload reduction)
Quick recap, part 2:
--Inflation pushes 🩸 into coronaries & raises systemic diastolic pressure (this is called diastolic augmentation)
--Deflation decreases aortic pressure & lowers systolic wall tension (afterload reduction)
17/28
Quick plug for more learning:
Here we are focusing on basics. (You have to walk before you run, right?)
To learn about the next level of IABP physiology, I *highly* recommend this review article by Morici et. al from @JCardFail
onlinejcf.com/article/S1071-…
Quick plug for more learning:
Here we are focusing on basics. (You have to walk before you run, right?)
To learn about the next level of IABP physiology, I *highly* recommend this review article by Morici et. al from @JCardFail
onlinejcf.com/article/S1071-…
18/28
There are 2 key concepts to understand when working with 🎈: timing & triggering
TIMING: when the 🎈 inflates & deflates in relation to the patient's cardiac cycle
TRIGGERING: signal used to identify key parts of the cardiac cycle to properly time 🎈 inflation & deflation
There are 2 key concepts to understand when working with 🎈: timing & triggering
TIMING: when the 🎈 inflates & deflates in relation to the patient's cardiac cycle
TRIGGERING: signal used to identify key parts of the cardiac cycle to properly time 🎈 inflation & deflation
19/28
More about timing:
--Inflation and deflation occur based on the cardiac cycle
--We assess this by looking at the arterial pressure waveform
More about timing:
--Inflation and deflation occur based on the cardiac cycle
--We assess this by looking at the arterial pressure waveform
20/28
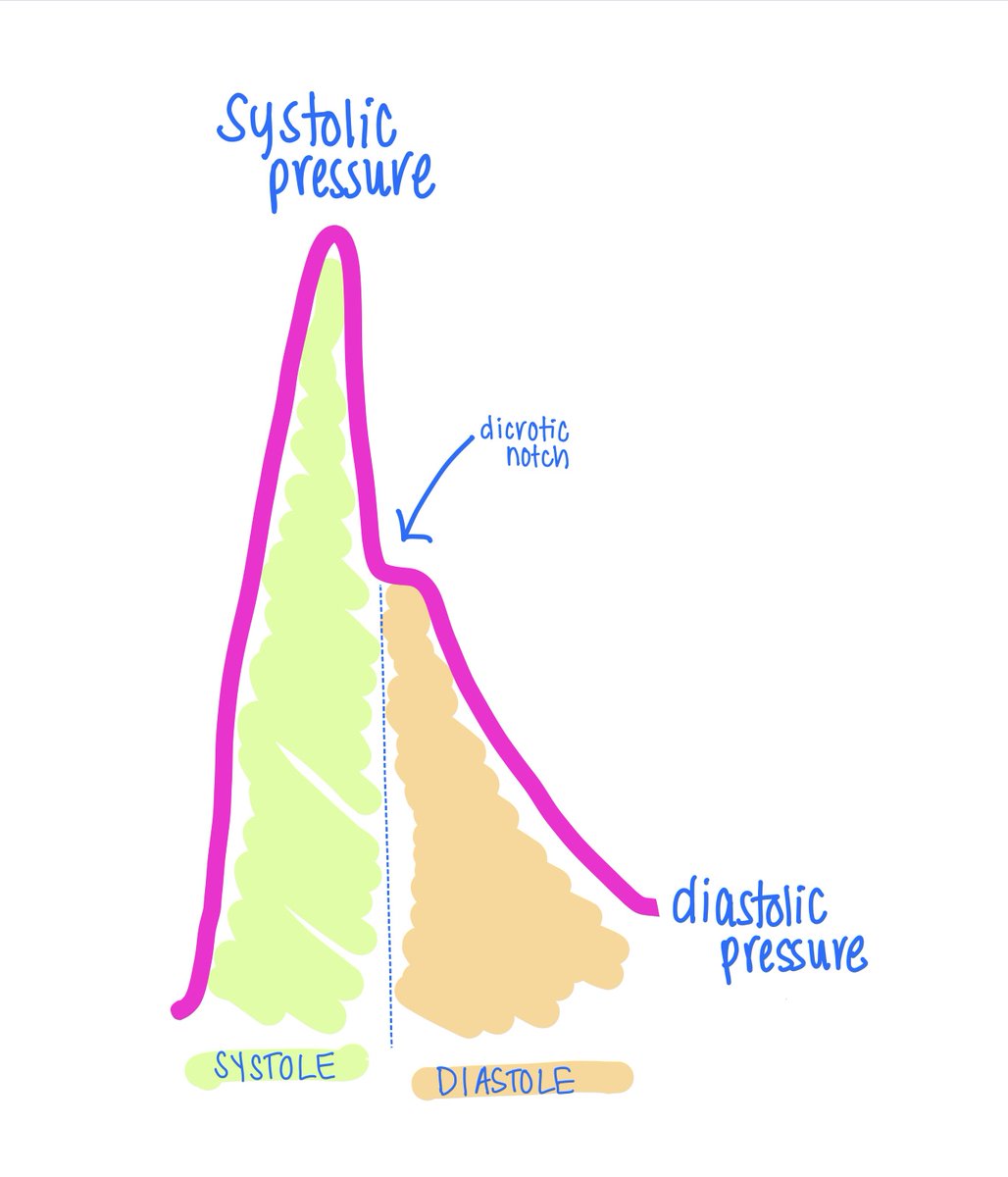
Let's first recall the normal arterial waveform which I drew below
Let's first recall the normal arterial waveform which I drew below
21/28
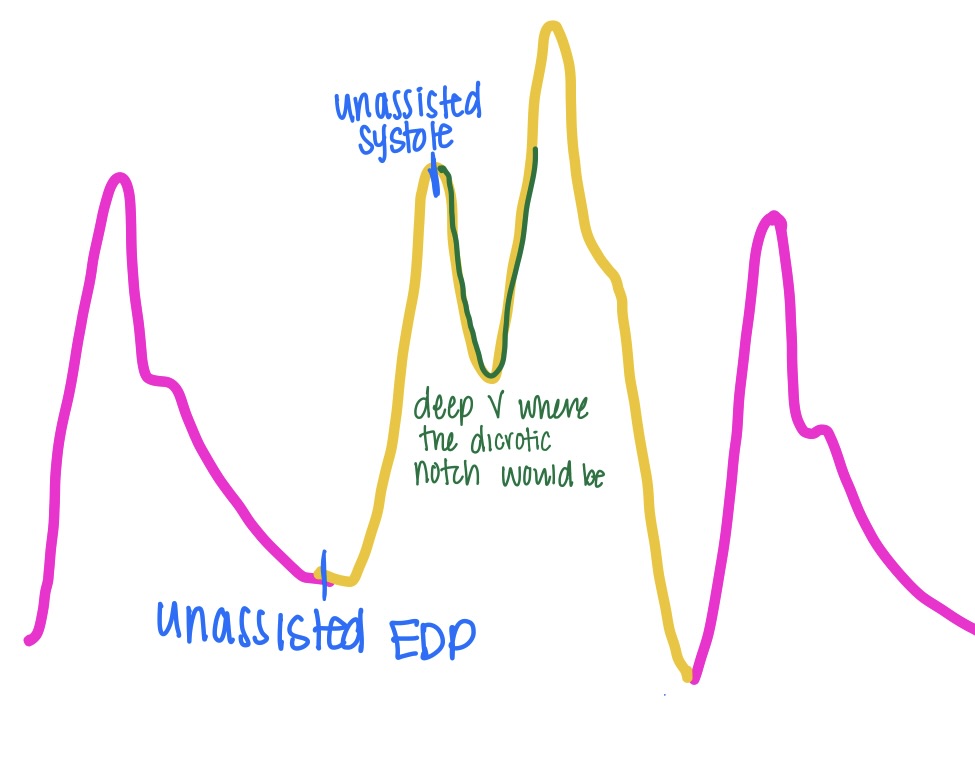
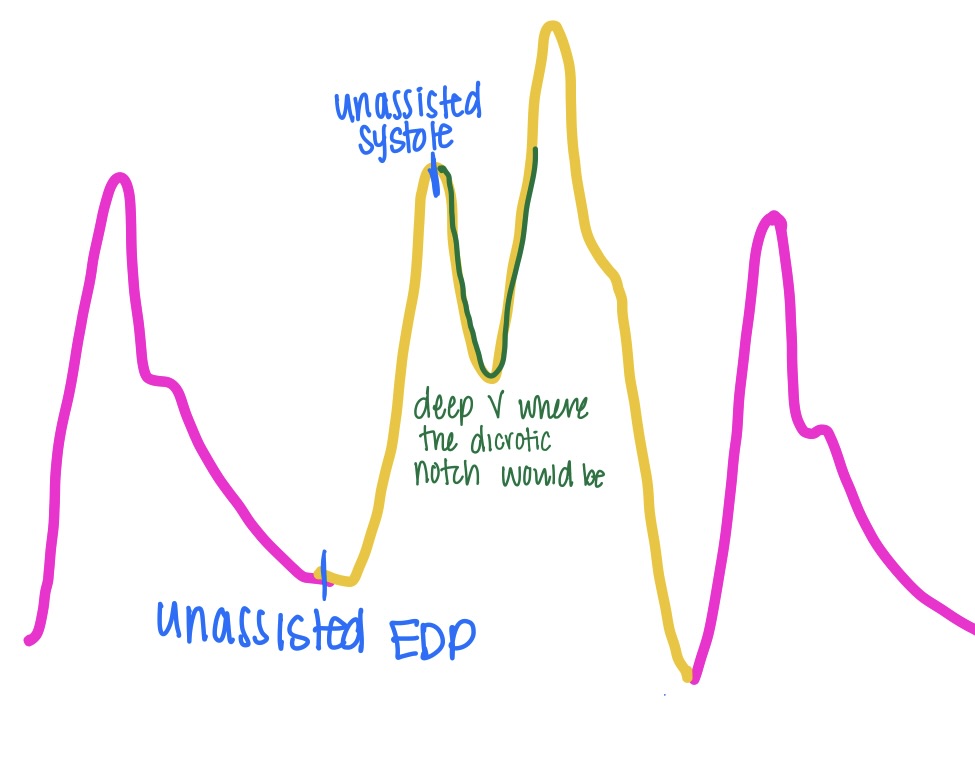
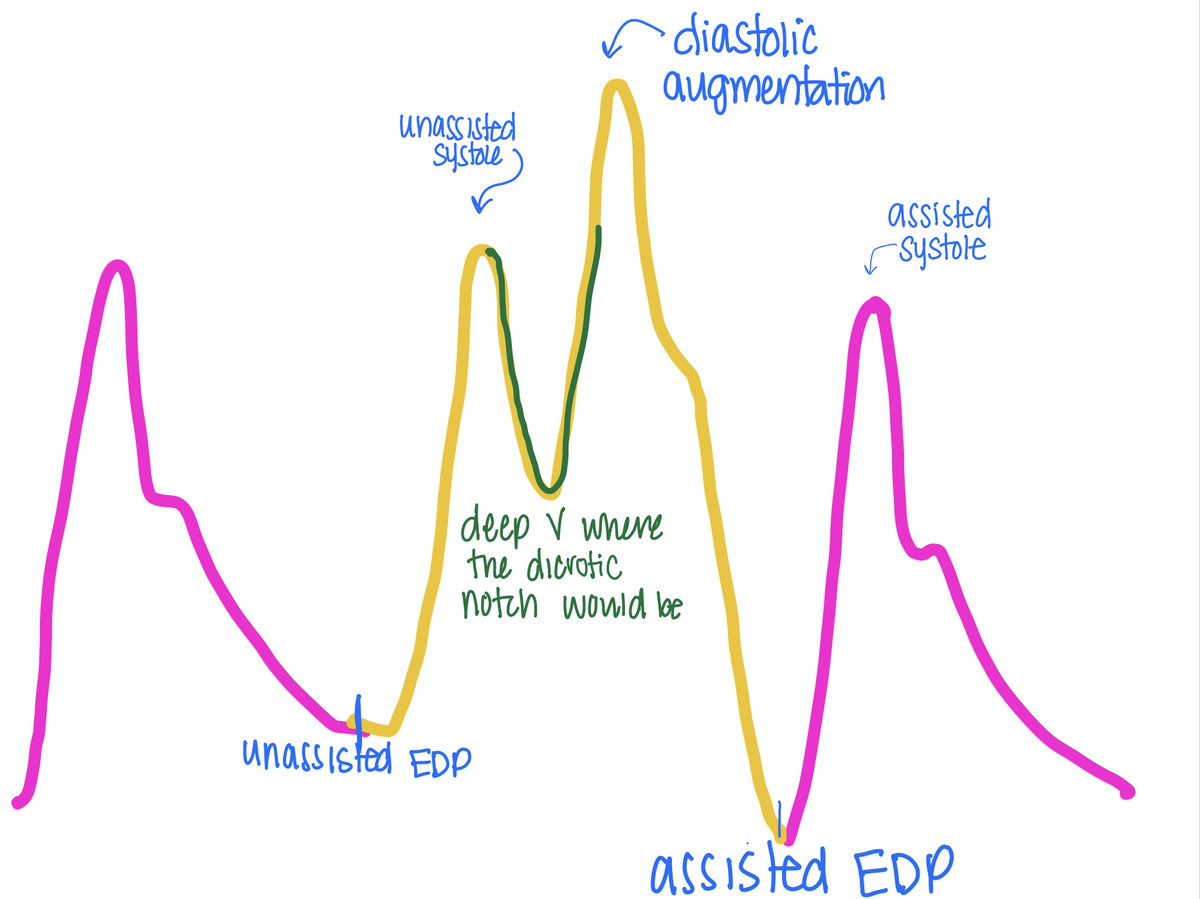
Remember, the the IABP inflates during diastole which starts at the dicrotic notch (see above)
🎈instead of the notch, you see a deep V which signifies rapid inflation of the balloon followed by an increase in diastolic pressure 🎈
Remember, the the IABP inflates during diastole which starts at the dicrotic notch (see above)
🎈instead of the notch, you see a deep V which signifies rapid inflation of the balloon followed by an increase in diastolic pressure 🎈
22/28
🎈 This is followed by diastolic augmentation, which should be higher than peak unassisted systole
🎈 Then, see reduction in aortic EDP (called assisted EDP)
🎈 Finally, see a decrease in systolic pressure (called assisted systole). This occurs in the next cycle at 1:1
🎈 This is followed by diastolic augmentation, which should be higher than peak unassisted systole
🎈 Then, see reduction in aortic EDP (called assisted EDP)
🎈 Finally, see a decrease in systolic pressure (called assisted systole). This occurs in the next cycle at 1:1
23/28
Recall that IABP can inflate/deflate at different intervals wrt the cardiac cycle: 1:1, 1:2, & 1:3
1:1 provides the most support because the IABP inflates and deflates with each cardiac cycle. But, to assess unassisted & assisted waveform, IABP needs to be at 1:2 or lower
Recall that IABP can inflate/deflate at different intervals wrt the cardiac cycle: 1:1, 1:2, & 1:3
1:1 provides the most support because the IABP inflates and deflates with each cardiac cycle. But, to assess unassisted & assisted waveform, IABP needs to be at 1:2 or lower
24/28
Check out this amazing "Devices in a Dash" video by @KatieV_MD & the @CardioNerds family.
Adult learning theory concept from "Make it Stick" - use the video as a form of "retrieval practice" by pausing the video & recalling different concepts. Space out your practice!
Check out this amazing "Devices in a Dash" video by @KatieV_MD & the @CardioNerds family.
Adult learning theory concept from "Make it Stick" - use the video as a form of "retrieval practice" by pausing the video & recalling different concepts. Space out your practice!
25/28
Now, triggering:
Trigger = event that the IABP sees and responds to in order to time inflation & deflation
There are multiple trigger options: EKG, pacer spikes, pressure waveform, & an "internal trigger." Most use "automatic mode" w/ combo of ECG & pressure triggering
Now, triggering:
Trigger = event that the IABP sees and responds to in order to time inflation & deflation
There are multiple trigger options: EKG, pacer spikes, pressure waveform, & an "internal trigger." Most use "automatic mode" w/ combo of ECG & pressure triggering
26/28
Whew! That was a lot. Thanks for going on this journey with me.
Key things I hope you got:
🎈What is an IABP
🎈Primary hemodynamic effects
🎈How IABP waveform differs from normal arterial waveform
📅 Next: trouble with timing
📅 Then: cases
Whew! That was a lot. Thanks for going on this journey with me.
Key things I hope you got:
🎈What is an IABP
🎈Primary hemodynamic effects
🎈How IABP waveform differs from normal arterial waveform
📅 Next: trouble with timing
📅 Then: cases
27/28
As always, it takes a village.
Shout out to @AndreaElliottUM for the inspiration, @KatieV_MD for the stellar edits, the entire @CardioNerds team for the support, and @ngaglianello & @rytanderson for answering my many (sometimes frantic) texts.
As always, it takes a village.
Shout out to @AndreaElliottUM for the inspiration, @KatieV_MD for the stellar edits, the entire @CardioNerds team for the support, and @ngaglianello & @rytanderson for answering my many (sometimes frantic) texts.
28/28
References:
🎈onlinejcf.com/article/S1071-…
🎈lms.getinge.training/lms/course/101…
🎈pubmed.ncbi.nlm.nih.gov/25348545/
🎈Amazing lecture by @AndreaElliottUM that I heard on the fellowship interview trail
🎈litfl.com/intra-aortic-b…
🎈journals.lww.com/anesthesia-ana…
🎈ncbi.nlm.nih.gov/pmc/articles/P…
References:
🎈onlinejcf.com/article/S1071-…
🎈lms.getinge.training/lms/course/101…
🎈pubmed.ncbi.nlm.nih.gov/25348545/
🎈Amazing lecture by @AndreaElliottUM that I heard on the fellowship interview trail
🎈litfl.com/intra-aortic-b…
🎈journals.lww.com/anesthesia-ana…
🎈ncbi.nlm.nih.gov/pmc/articles/P…
• • •
Missing some Tweet in this thread? You can try to
force a refresh



