Day 3 @covidinquiryuk
🚨Prof David Heymann
CV highlights
2003: WHO executive director for communicable diseases - headed the global response to SARS
2017-2022: Chair of the WHO Strategic & Technical Advisory Committee on Infectious Hazards (STAG-IH)
Written evidence 🥁
/1
🚨Prof David Heymann
CV highlights
2003: WHO executive director for communicable diseases - headed the global response to SARS
2017-2022: Chair of the WHO Strategic & Technical Advisory Committee on Infectious Hazards (STAG-IH)
Written evidence 🥁
/1
Annex 2: Matters to be addressed from Letter of
Instruction
I hope you don't mind, but for obvious reasons I'll focus on his comments on transmission
#COVIDisAirborne
/2
Instruction
I hope you don't mind, but for obvious reasons I'll focus on his comments on transmission
#COVIDisAirborne
/2

Transmission: pt 71 onwards
'Researchers addressed major questions about transmission of SARS-CoV-2 during the first months of the pandemic
It was known...that the virus spread easily...especially in indoor & other closed spaces such as the Diamond Princess cruise ship...
/3
'Researchers addressed major questions about transmission of SARS-CoV-2 during the first months of the pandemic
It was known...that the virus spread easily...especially in indoor & other closed spaces such as the Diamond Princess cruise ship...
/3
...in what appeared to be superspreading events
[superspreading = a hallmark of airborne transmission, obvs]
Prof H continues:
'As a result the question was raised as to whether it was spread by aerosol particles, or whether infection was transmitted from human to human...
/4
[superspreading = a hallmark of airborne transmission, obvs]
Prof H continues:
'As a result the question was raised as to whether it was spread by aerosol particles, or whether infection was transmitted from human to human...
/4
only by droplets as had occurred in some SARS infections, & as appears to be the predominant means of transmission in MERS; & whether fomites (objects or materials that are contaminated with droplets containing infectious virus) played a role in transmission'
Wait for it...
/5
Wait for it...
/5
'Both droplets & aerosol particles contain virus surrounded by moisture - mucus, saliva and/or water
It was known for other respiratory infections...that transmission could occur...when droplets & aerosol particles spread from a cough or sneeze & also by voice projection...
/6
It was known for other respiratory infections...that transmission could occur...when droplets & aerosol particles spread from a cough or sneeze & also by voice projection...
/6

'Early studies in China suggested that the SARS-CoV-2 could be transmitted by aerosols as well as by droplets'
🚨Jan 2020
He's mentioned the bus, @LazarusLong13 @EvonneTCurran!
The clever droplet flying backwards 5m & causing infection - NOT
#COVIDisAirborne Jan 2020: FIN
/7
🚨Jan 2020
He's mentioned the bus, @LazarusLong13 @EvonneTCurran!
The clever droplet flying backwards 5m & causing infection - NOT
#COVIDisAirborne Jan 2020: FIN
/7

& look @jljcolorado, Prof Heymann goes on to mention the Skagit county superspreading choir event as further early 2020 evidence of aerosol transmission
But: he clearly sees the word airborne as a WHO hot potato - he only mentions it in the context of IPC guidance during AGPs
8
But: he clearly sees the word airborne as a WHO hot potato - he only mentions it in the context of IPC guidance during AGPs
8

Point 80: He probably thinks he's being clever here though, suggesting a problem with terminology as a reason for WHO, PHE, CDC et al allowing HCWs to go to their deaths thanks to the restriction of N95/FFP3 to AGPs
But he's forgotten THE PRECAUTIONARY PRINCIPLE
/9
But he's forgotten THE PRECAUTIONARY PRINCIPLE
/9

In fact @mdc_martinus isn't it true that WHO IPC guidance for pathogens with pandemic potential require adherence to the PRECAUTIONARY PRINCIPLE until modes of transmission are definitively ascertained?
🚨IPC guidance authors should NEVER have deprived HCWs of this PPE QED
10
🚨IPC guidance authors should NEVER have deprived HCWs of this PPE QED
10

Coming in to land on this one...
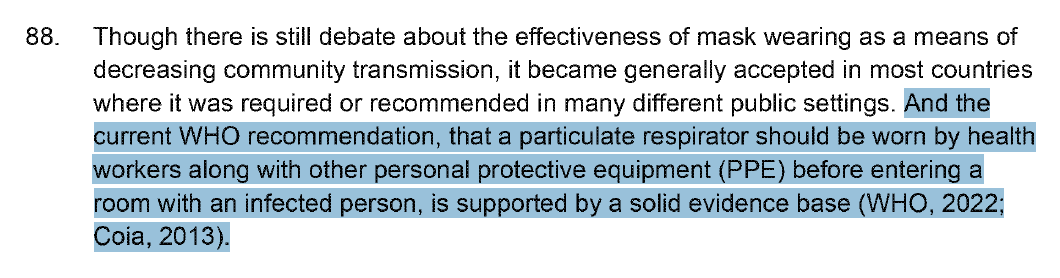
Strength of evidence underlying benefits of community mask wearing is stated to change over time - 'unreserved recommendation' by WHO, Dec 2022
& dear gaslit by all Gov-linked agencies HCW readers, please note the last sentence, point 88...
/11
Strength of evidence underlying benefits of community mask wearing is stated to change over time - 'unreserved recommendation' by WHO, Dec 2022
& dear gaslit by all Gov-linked agencies HCW readers, please note the last sentence, point 88...
/11

'& the current WHO recommendation, that a particulate respirator should be worn by health workers along with other PPE before entering a room with an infected person, is supported by a solid evidence base (WHO, 2022; Coia, 2013)'
What's my point?
/12
What's my point?
/12
Well the obvious one is that UK IPC leadership is so deranged, that the infection control manual mandated for use by all NHS providers states that SARS2 is only airborne transmitted during AGPs
It's a droplet transmitted disease in UK hospitals, don't you know?
Is 🌏 flat, too?
It's a droplet transmitted disease in UK hospitals, don't you know?
Is 🌏 flat, too?
But check out the reference Prof Heymann uses to affirm the 'solid evidence base' for particulate respirators: includes Coia et al
IPC authors, SAGE, NERVTAG, CMO, CSA are clearly in a hole after this evidence alone, but Heymann further dumps them in it by using JVTs own paper!
IPC authors, SAGE, NERVTAG, CMO, CSA are clearly in a hole after this evidence alone, but Heymann further dumps them in it by using JVTs own paper!

🚨Summary
SARS2 was known to be airborne in Jan 2020: when did you know?
Vague & unconvincing statements about the need for clearer terminology don't stack up against the complete abandonment of WHO's own precautionary principle
HCWs were shafted, & died caring for others
/15
SARS2 was known to be airborne in Jan 2020: when did you know?
Vague & unconvincing statements about the need for clearer terminology don't stack up against the complete abandonment of WHO's own precautionary principle
HCWs were shafted, & died caring for others
/15
Millions more were infected, & died, thanks to WHO's inability to say the word 'airborne' & state an empirical truth they knew to be correct, in Jan 2020, loud & clear
#CovidIsAirborne
Bring on the UK 'scientist experts' to wriggle on the hook & claim they did not know
End
#CovidIsAirborne
Bring on the UK 'scientist experts' to wriggle on the hook & claim they did not know
End
Link to Prof Heymann's written evidence
covid19.public-inquiry.uk/wp-content/upl…
covid19.public-inquiry.uk/wp-content/upl…
• • •
Missing some Tweet in this thread? You can try to
force a refresh