
Lots of inane comments from Elon/Rohan bros that vaccines don’t prevent disease.
Let’s debunk these claims:
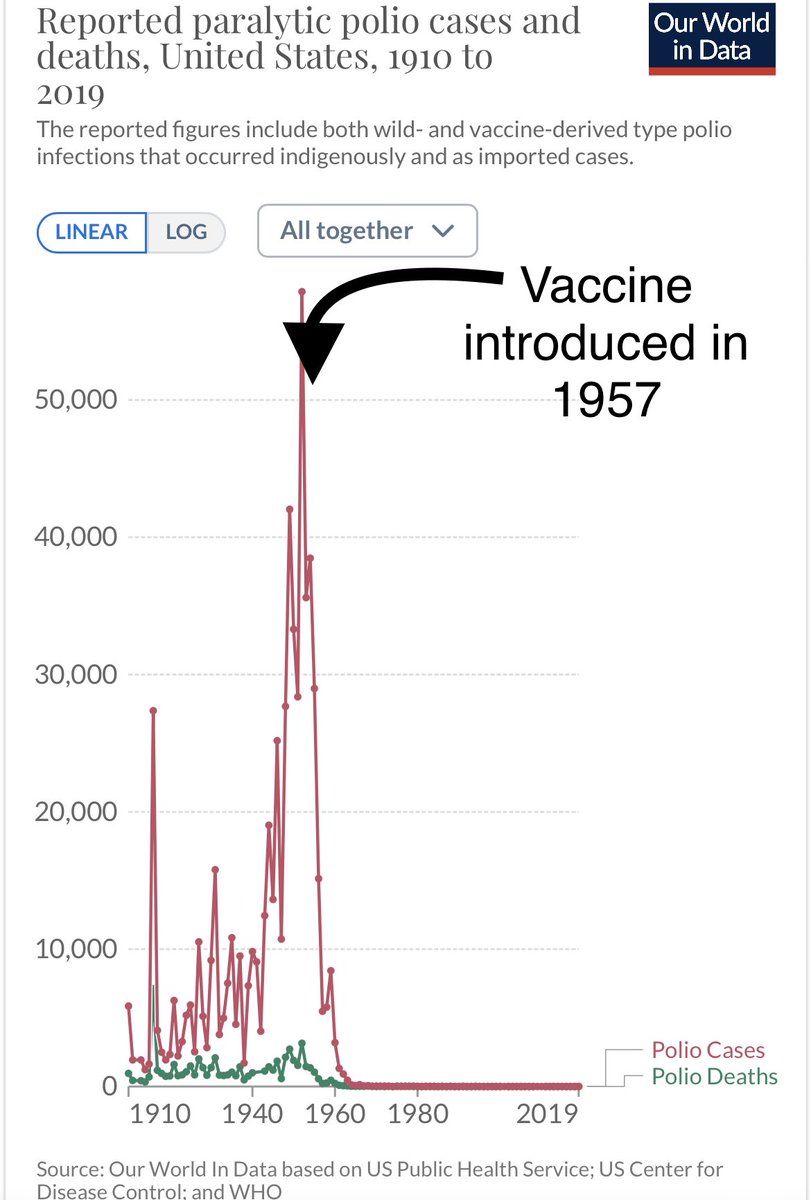
1. Polio - vaccine introduced 1957
ourworldindata.org/grapher/report…
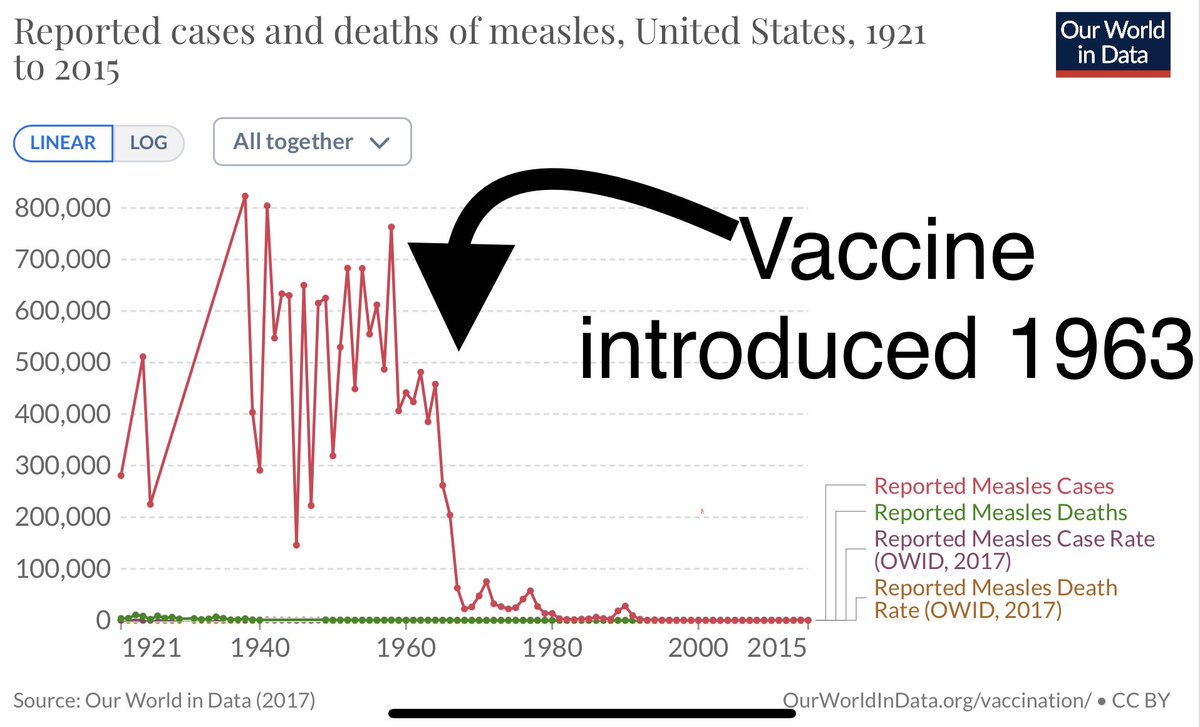
2. Measles - vaccine introduced 1963
ourworldindata.org/grapher/measle…
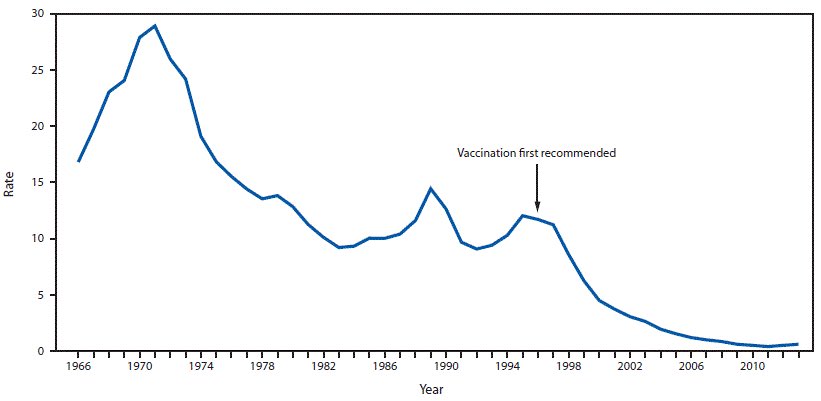
Let’s debunk these claims:
1. Polio - vaccine introduced 1957
ourworldindata.org/grapher/report…
2. Measles - vaccine introduced 1963
ourworldindata.org/grapher/measle…



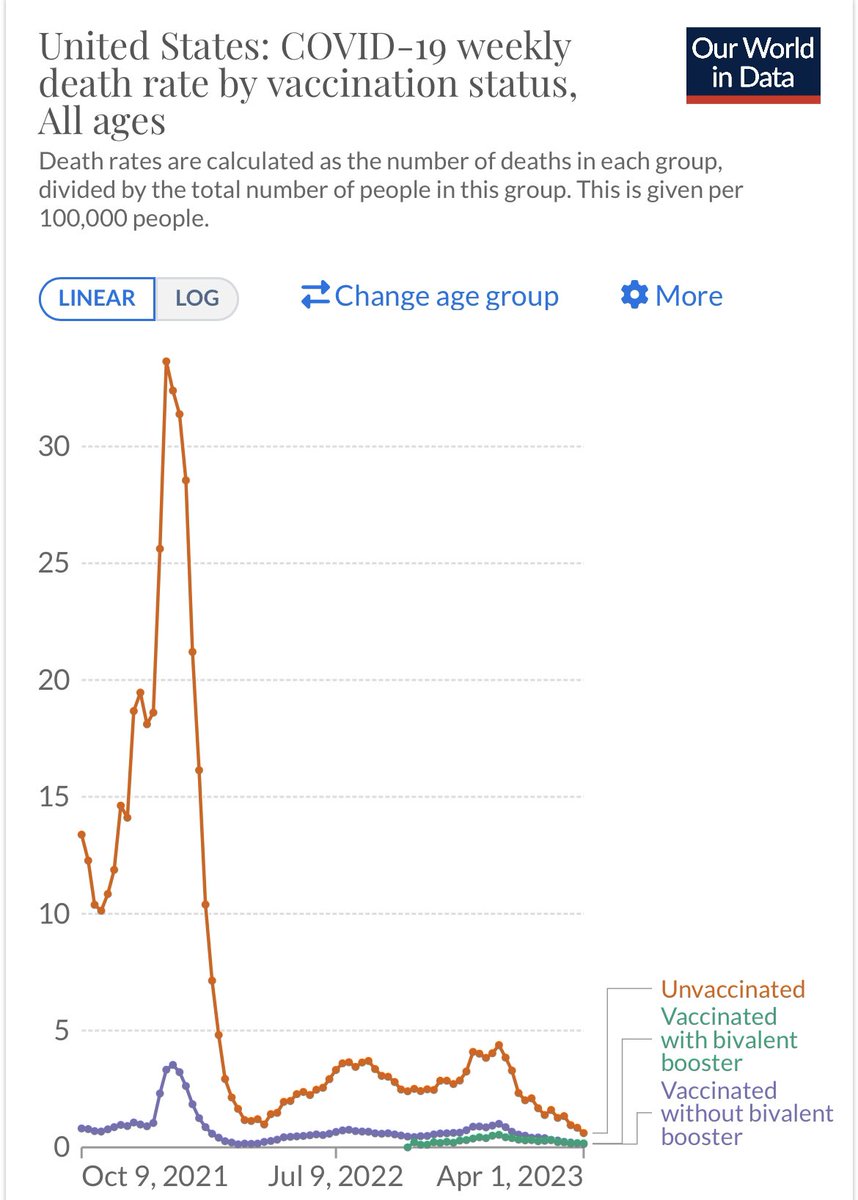
Lots of tin foil hat folks acknowledge that COVID deaths are reduced by the vaccine but claim an increase in all cause mortality.
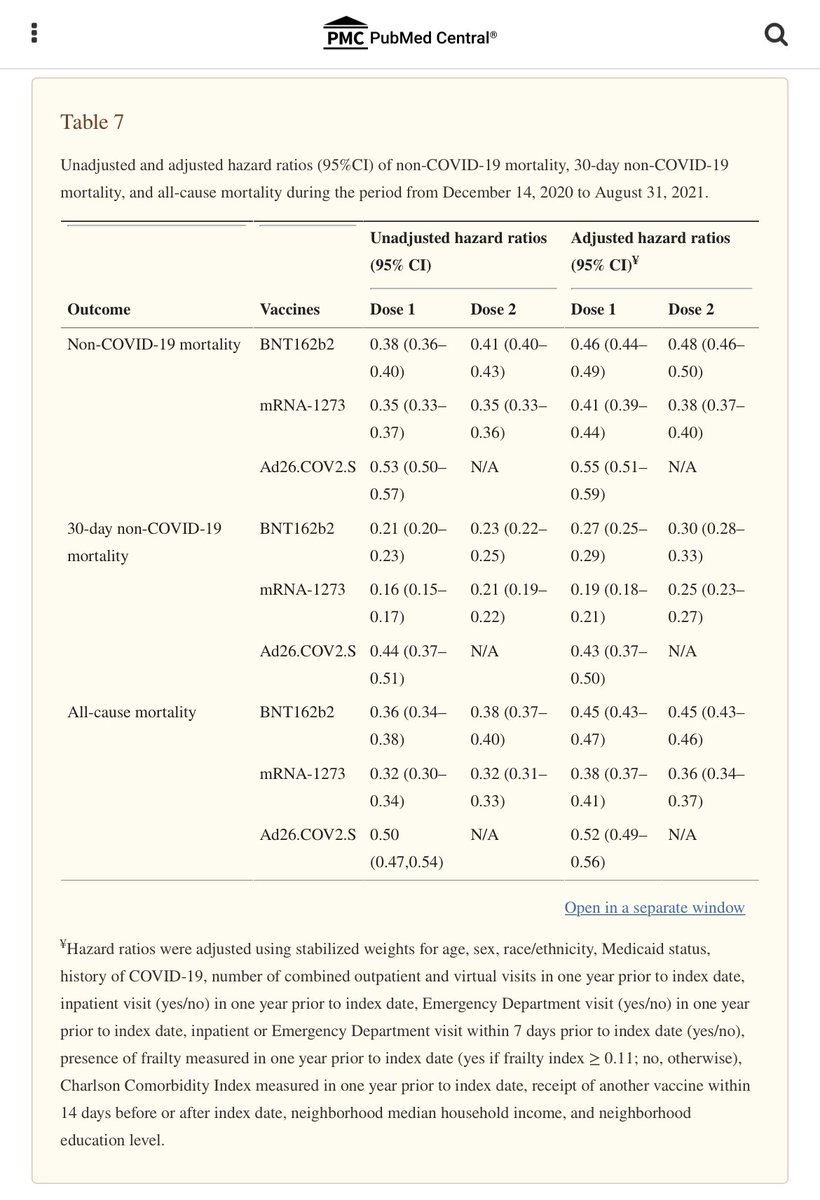
In fact the opposite is true: COVID vaccination was associated with LOWER all cause mortality & non-COVID mortality.
ncbi.nlm.nih.gov/pmc/articles/P…
In fact the opposite is true: COVID vaccination was associated with LOWER all cause mortality & non-COVID mortality.
ncbi.nlm.nih.gov/pmc/articles/P…
• • •
Missing some Tweet in this thread? You can try to
force a refresh































