📄 20 studies that Internal Medicine Residents should read in the first year 👇
1/ 🏃♀️ RACE II trial: Lenient resting HR < 110 was non-inferior to a strict HR < 80 in patients with atrial fibrillation.
🧵
1/ 🏃♀️ RACE II trial: Lenient resting HR < 110 was non-inferior to a strict HR < 80 in patients with atrial fibrillation.
🧵
2/🧂SALT-ED trial: one of the reasons I prefer LR > NS
⚠️Balanced crystalloids (LR, Plasma-Lyte) does not reduce duration of hospitalization when compared to NS. However, balanced crystalloid use is associated with a reduction in major kidney-related events.
⚠️Balanced crystalloids (LR, Plasma-Lyte) does not reduce duration of hospitalization when compared to NS. However, balanced crystalloid use is associated with a reduction in major kidney-related events.
3/ 🦠 Surviving Sepsis Guidelines
❗️Fluids
❗️Antibiotics timing
❗️Vasoactive agents
❗️Lactic acid
❗️Fluids
❗️Antibiotics timing
❗️Vasoactive agents
❗️Lactic acid

4/ 🫁 ARDSNet: Standard of care - Tidal volume 6cc/kg of IDEAL BODY WEIGHT —> Lower mortality; More ventilator free days in ARDS patients
- Results are extrapolated to the safe ventilation of non-ARDS patients as well
- Results are extrapolated to the safe ventilation of non-ARDS patients as well

5/ 🩻REDUCE trial: Steroids use in COPD Exacerbation
Definitely, the most cited GMF trial
⚠️ A 5-day course of glucocorticoids is non-inferior to a 14-day course for treatment of acute COPD exacerbations in prevention of re-exacerbations.
Definitely, the most cited GMF trial
⚠️ A 5-day course of glucocorticoids is non-inferior to a 14-day course for treatment of acute COPD exacerbations in prevention of re-exacerbations.
6/ 🧠 CHANCE trial
⚠️Among patients with acute TIA or minor ischemic stroke, starting aspirin/clopidogrel within 24h of symptom onset reduces the 90-day stroke incidence without increasing bleeding rates, when compared to aspirin monotherapy.
⚠️Among patients with acute TIA or minor ischemic stroke, starting aspirin/clopidogrel within 24h of symptom onset reduces the 90-day stroke incidence without increasing bleeding rates, when compared to aspirin monotherapy.

7/ 💊 Amazing Editorial on ASA In Primary Prophylaxis
Personalized approach but not favored per ASCEND (2018), ARRIVE (2018), and ASPREE (2018) trials
Personalized approach but not favored per ASCEND (2018), ARRIVE (2018), and ASPREE (2018) trials

8/ 🫀DAPA-HF: Favorite trial by every cardiologist since Dapa showed a mortality benefits
⚠️In HFrEF (NYHA II-IV, LVEF ≤40%) with or without T2DM, the addition of the SGLT-2 inhibitor dapagliflozin decreased rates of CV death or worsening HF, as well as all-cause mortality.
⚠️In HFrEF (NYHA II-IV, LVEF ≤40%) with or without T2DM, the addition of the SGLT-2 inhibitor dapagliflozin decreased rates of CV death or worsening HF, as well as all-cause mortality.
9/ 🏥 How to treat hypertensive urgency!
⚠️Important article! Urgency is not an emergency! Don’t treat with IV meds!
⚠️Important article! Urgency is not an emergency! Don’t treat with IV meds!

10/ 🍬 NICE-SUGAR trial: 140-180 superior than more aggressive BS goals
⚠️Reason why we target glucose of 140-180 in the hospital settings
⚠️Reason why we target glucose of 140-180 in the hospital settings
11/ 💊 COURAGE-Trial: TO PCI OR NOT TO PCI
⚠️ In patients with stable CAD, there were no differences in death and MI between optimal medical therapy plus PCI vs. OMT alone.
⚠️ In patients with stable CAD, there were no differences in death and MI between optimal medical therapy plus PCI vs. OMT alone.
12/ ❤️🔥AFFIRM trial
⚠️ In patients with nonvalvular AF, there is no survival benefit between rate and rhythm control, but rhythm trends toward increased mortality.
‼️EAST-AFNET 4 trial is a newer trial: early rhythm-control strategy was associated with a favorable outcomes
⚠️ In patients with nonvalvular AF, there is no survival benefit between rate and rhythm control, but rhythm trends toward increased mortality.
‼️EAST-AFNET 4 trial is a newer trial: early rhythm-control strategy was associated with a favorable outcomes
13/ 🧠 POINT trial
⚠️ Acute TIA or minor ischemic stroke, starting aspirin/clopidogrel within 12h of symptom onset reduces the 90-day stroke incidence at the cost of increasing bleeding rates, when compared to aspirin monotherapy.
⚠️ Acute TIA or minor ischemic stroke, starting aspirin/clopidogrel within 12h of symptom onset reduces the 90-day stroke incidence at the cost of increasing bleeding rates, when compared to aspirin monotherapy.
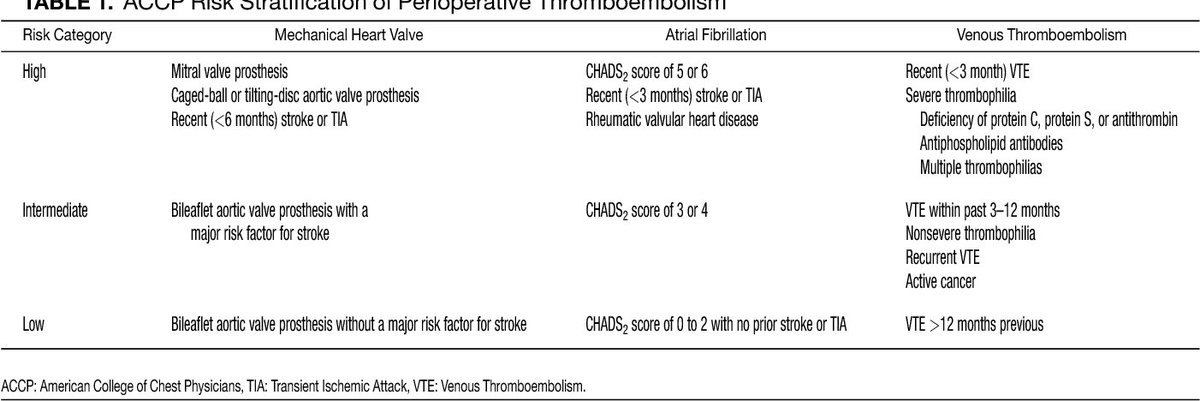
14/ 🔪 BRIDGE trial
⚠️Atrial fibrillation pts receiving anticoagulation and undergoing an invasive procedure, periprocedural bridging with LMWH did not reduce the incidence of arterial thromboembolism when compared to no bridging, but did increase the risk of major bleeding.
⚠️Atrial fibrillation pts receiving anticoagulation and undergoing an invasive procedure, periprocedural bridging with LMWH did not reduce the incidence of arterial thromboembolism when compared to no bridging, but did increase the risk of major bleeding.
15/ 🛏️ PROSEVA trial
⚠️ Among patients with severe ARDS (P:F ratio <150 mm Hg), prone positioning reduces 28-day mortality.
⚠️ Among patients with severe ARDS (P:F ratio <150 mm Hg), prone positioning reduces 28-day mortality.
16/ 💩 Fidaxomicin vs Oral Vancomycin in C.diff infection
⚠️ Fidaxomicin was noninferior to vancomycin in achieving rates of clinical cure among patients with Clostridium difficile-associated diarrhea and resulted in fewer recurrent infections.
⚠️ Fidaxomicin was noninferior to vancomycin in achieving rates of clinical cure among patients with Clostridium difficile-associated diarrhea and resulted in fewer recurrent infections.
17/ 🫘 DOSE trial
⚠️ Among patients with acute decompensated HF, high-dose loop diuretics are associated with better symptom improvement than low-dose loop at the cost of some renal impairment, while continuous diuretic infusions are no better than intermittent diuretic boluses
⚠️ Among patients with acute decompensated HF, high-dose loop diuretics are associated with better symptom improvement than low-dose loop at the cost of some renal impairment, while continuous diuretic infusions are no better than intermittent diuretic boluses
18/ 💧SAFE study: Albumin vs NS
⚠️ Albumin and normal saline result in similar clinical outcomes when administered to ICU patients for volume resuscitation, except for those with traumatic brain injury who do worse with albumin.
⚠️ Albumin and normal saline result in similar clinical outcomes when administered to ICU patients for volume resuscitation, except for those with traumatic brain injury who do worse with albumin.

19/ 💊 ROCKET-AF trial
⚠️ Among patients with nonvalvular atrial fibrillation, rivaroxaban is noninferior to warfarin in preventing stroke and systemic thromboembolism.
⚠️ Among patients with nonvalvular atrial fibrillation, rivaroxaban is noninferior to warfarin in preventing stroke and systemic thromboembolism.
20/ 🩸 Urgent vs Early Endoscopy for AUIB
⚠️ Endoscopy performed within 6 hours after gastroenterologic consultation was not associated with lower 30-day mortality than endoscopy performed between 6 and 24 hours after consultation.
⚠️ Endoscopy performed within 6 hours after gastroenterologic consultation was not associated with lower 30-day mortality than endoscopy performed between 6 and 24 hours after consultation.
#MedTwitter #MedEd #IMG
Sources: @NEJM @JAMA_current @JAMAInternalMed @yourICM
Please add if I missed something.
Sources: @NEJM @JAMA_current @JAMAInternalMed @yourICM
Please add if I missed something.
• • •
Missing some Tweet in this thread? You can try to
force a refresh