1/37
Back for IABP basics pt 2, @CardioNerds style!
AKA things I've gotten wrong on rounds so you don't have to, round 2.
ICYMI, check out the first tweetorial for background. (Thanks for the unexpectedly awesome response!)
Today we'll discuss timing & triggering Ready? Go!🚦
Back for IABP basics pt 2, @CardioNerds style!
AKA things I've gotten wrong on rounds so you don't have to, round 2.
ICYMI, check out the first tweetorial for background. (Thanks for the unexpectedly awesome response!)
Today we'll discuss timing & triggering Ready? Go!🚦
@CardioNerds 2/37
First, let's do some spaced repetition & retrieval practice.
When in the cardiac cycle does an IABP inflate and deflate?
First, let's do some spaced repetition & retrieval practice.
When in the cardiac cycle does an IABP inflate and deflate?
@CardioNerds 3/37
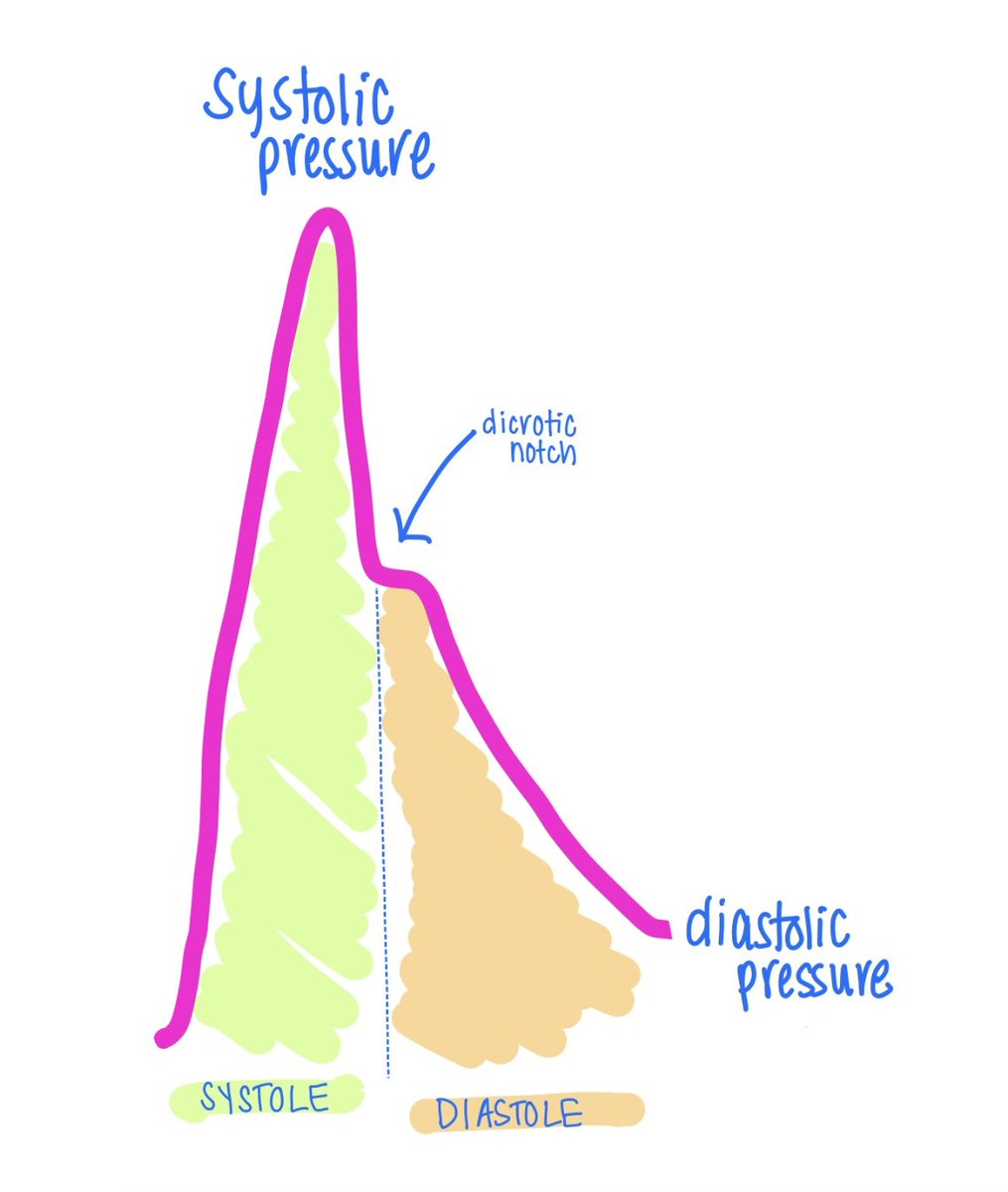
Next, when looking at a NORMAL arterial waveform, at what point does diastole start?
Next, when looking at a NORMAL arterial waveform, at what point does diastole start?
@CardioNerds 4/37
Which of the following hemodynamic effects is NOT seen with a normally functioning IABP?
Which of the following hemodynamic effects is NOT seen with a normally functioning IABP?
5/37
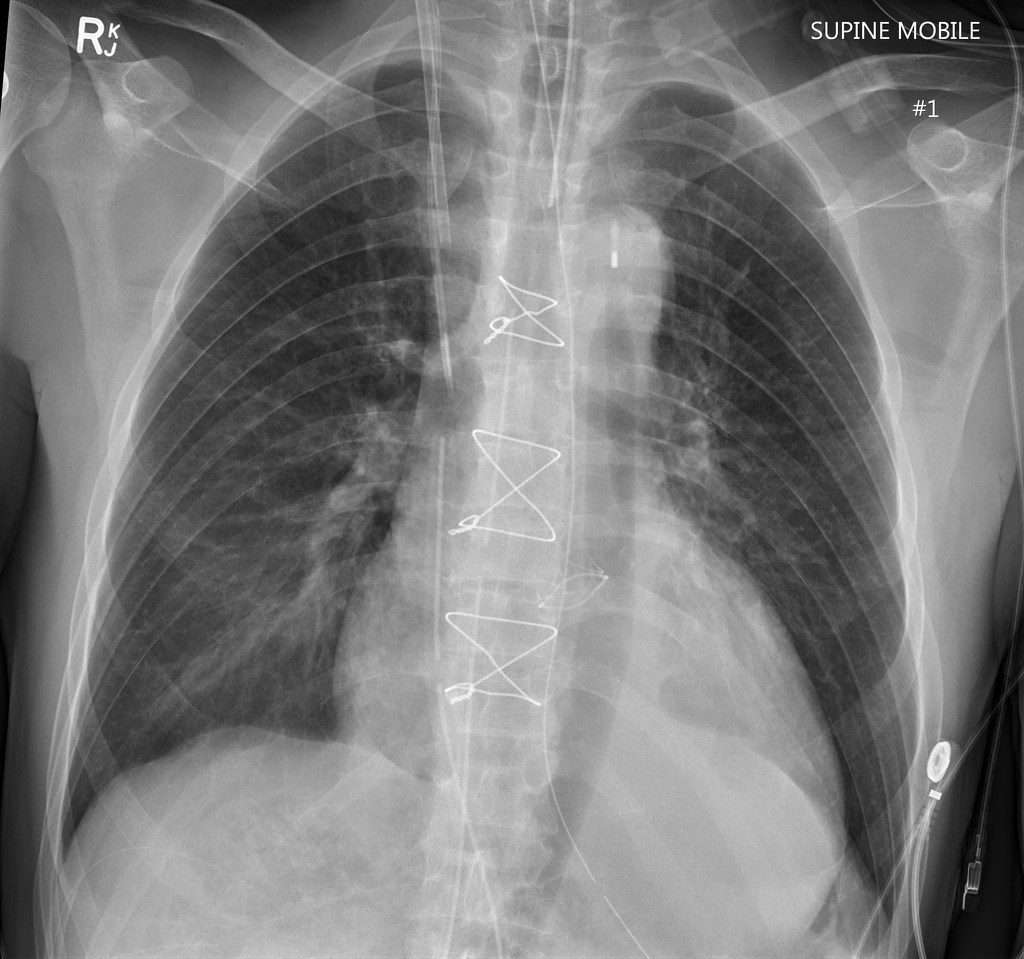
Q: Is this IABP positioned correctly? Why or why not?
👀 Answer in next tweet 👀
Q: Is this IABP positioned correctly? Why or why not?
👀 Answer in next tweet 👀
6/37
A: It is too high!
Should be ~2cm above the carina on CXR.....this is definitely higher
Risk with this positioning: occlude subclavian arteries
For fun: what is the risk if the IABP is too low?
....occludes the renal arteries
A: It is too high!
Should be ~2cm above the carina on CXR.....this is definitely higher
Risk with this positioning: occlude subclavian arteries
For fun: what is the risk if the IABP is too low?
....occludes the renal arteries
7/37
Now, quick review of nl 🎈waveform (1:2)
Inflation in diastole ➡️ diastolic augmentation (should be > than peak unassisted systole) ➡️ decreased LVEDP (aka assisted EDP) & decreased systolic pressure (aka assisted systole)
The 🎈 inflates at the site of the dicrotic notch
Now, quick review of nl 🎈waveform (1:2)
Inflation in diastole ➡️ diastolic augmentation (should be > than peak unassisted systole) ➡️ decreased LVEDP (aka assisted EDP) & decreased systolic pressure (aka assisted systole)
The 🎈 inflates at the site of the dicrotic notch

8/37
Ok, got it? Cool. Onwards.
In what situations would diastolic augmentation be insufficient? We can make a schema for this, splitting it up into three buckets:
🪣 Physiology issues
🪣 Mechanical issues
🪣 Balloon timing issues
Ok, got it? Cool. Onwards.
In what situations would diastolic augmentation be insufficient? We can make a schema for this, splitting it up into three buckets:
🪣 Physiology issues
🪣 Mechanical issues
🪣 Balloon timing issues
9/37
🪣: Physiology issues
- Vasodilatory states (the IABP is relatively undersized, & therefore it lacks a good vacuum effect with deflation)
- Tachycardia
- Hypovolemia
- Essentially any time when stroke volume is too low (eg. aortic insufficiency)
🪣: Physiology issues
- Vasodilatory states (the IABP is relatively undersized, & therefore it lacks a good vacuum effect with deflation)
- Tachycardia
- Hypovolemia
- Essentially any time when stroke volume is too low (eg. aortic insufficiency)
10/37
🪣: Mechanical issues
(🚨= emergency)
- Improper size
- Catheter kink
- Positioning (too high or too low)
- Leak, &/or too little helium in the balloon 🚨
- Balloon rupture (may see blood in tubing) 🚨
- Basically, any mechanical factor that impacts the balloon or catheter
🪣: Mechanical issues
(🚨= emergency)
- Improper size
- Catheter kink
- Positioning (too high or too low)
- Leak, &/or too little helium in the balloon 🚨
- Balloon rupture (may see blood in tubing) 🚨
- Basically, any mechanical factor that impacts the balloon or catheter
11/37
🪣: Balloon timing issues
-- Early deflation
-- Late deflation
-- Early inflation
-- Late inflation
Let's take a deeper dive into problems with timing.
🪣: Balloon timing issues
-- Early deflation
-- Late deflation
-- Early inflation
-- Late inflation
Let's take a deeper dive into problems with timing.
12/37
⏰ TIMING ⏰
In general, to assess timing the 🎈 should be at 1:2 so you can clearly see the difference between assisted & unassisted beats.
The worst timing errors are those when those balloon is inflated in systole: early inflation and late deflation.
⏰ TIMING ⏰
In general, to assess timing the 🎈 should be at 1:2 so you can clearly see the difference between assisted & unassisted beats.
The worst timing errors are those when those balloon is inflated in systole: early inflation and late deflation.
13/37
Early inflation = balloon inflates early (before the aortic valve is closed)
Problem?
Aortic pressure increases too soon ➡️ AV closes before LV empty ➡️ increased LVEDP, LVEDV, & LV afterload ➡️ badness (increase in LV work, O2 demand, & LV filling pressures & 🫁-edema )
Early inflation = balloon inflates early (before the aortic valve is closed)
Problem?
Aortic pressure increases too soon ➡️ AV closes before LV empty ➡️ increased LVEDP, LVEDV, & LV afterload ➡️ badness (increase in LV work, O2 demand, & LV filling pressures & 🫁-edema )
14/37
Early inflation is one of the worst timing errors because of the increase in afterload, which makes the heart work harder
How can you identify early inflation?
Inflation on assisted beat occurs before dicrotic notch
Early inflation is one of the worst timing errors because of the increase in afterload, which makes the heart work harder
How can you identify early inflation?
Inflation on assisted beat occurs before dicrotic notch

15/37
Next is late inflation = balloon inflates too late (after AV closes)
Problem?
Inflation when the ❤️ is already in diastole, so you don't see maximal ⬆️ in coronary perfusion & you get ⬇️ diastolic aug.
This means the 🎈 is less effective & get less improvement in CPP
Next is late inflation = balloon inflates too late (after AV closes)
Problem?
Inflation when the ❤️ is already in diastole, so you don't see maximal ⬆️ in coronary perfusion & you get ⬇️ diastolic aug.
This means the 🎈 is less effective & get less improvement in CPP
16/37
How to identify late inflation?
See the balloon inflation upstroke AFTER the dicrotic notch
How to identify late inflation?
See the balloon inflation upstroke AFTER the dicrotic notch

17/37
Ok, now on to early deflation = balloon delates early (during diastole)
Problem?
No suction event ➡️ suboptimal afterload reduction, increase in cardiac work, & increase in O2 demand which can worsen ischemia. Can also get retrograde coronary blood flow.
Ok, now on to early deflation = balloon delates early (during diastole)
Problem?
No suction event ➡️ suboptimal afterload reduction, increase in cardiac work, & increase in O2 demand which can worsen ischemia. Can also get retrograde coronary blood flow.
18/37
How to identify early deflation?
Assisted systole is >/= unassisted systole because it's not getting enough support (remember, it should be less than unassisted systole)
How to identify early deflation?
Assisted systole is >/= unassisted systole because it's not getting enough support (remember, it should be less than unassisted systole)

19/37
Finally, late deflation = balloon deflates too late (during systole when AV open)
Problem?
Trying to eject🩸 against inflated balloon ➡️ increase afterload & myocardial O2 demand/consumption. Can also ➡️ reduction in cardiac output & increase LV filling pressures
Finally, late deflation = balloon deflates too late (during systole when AV open)
Problem?
Trying to eject🩸 against inflated balloon ➡️ increase afterload & myocardial O2 demand/consumption. Can also ➡️ reduction in cardiac output & increase LV filling pressures
20/37
How to identify late deflation?
Wide diastolic augmentation, prolonged slope of assisted systole, assisted EDP may be = unassisted EDP (remember, assisted EDP should be lower than unassisted EDP)
How to identify late deflation?
Wide diastolic augmentation, prolonged slope of assisted systole, assisted EDP may be = unassisted EDP (remember, assisted EDP should be lower than unassisted EDP)

21/37
We're done with the basics of timing!
Let's take a quick pause and review some 🔑 points:
1. Remember your buckets: physiology, mechanical, or timing
2. If timing problem, look at waveform to determine if problem with inflation or deflation, and if early or late
We're done with the basics of timing!
Let's take a quick pause and review some 🔑 points:
1. Remember your buckets: physiology, mechanical, or timing
2. If timing problem, look at waveform to determine if problem with inflation or deflation, and if early or late
22/37
Now for some high yield learning points about triggering.
🤷🏻♀️ WHAT? The trigger is what tells the balloon to inflate and deflate. Y
🤷🏻♀️ HOW? You set the trigger source. There are many options, but we'll focus on the 2 most common: EKG & pressure triggering.
Now for some high yield learning points about triggering.
🤷🏻♀️ WHAT? The trigger is what tells the balloon to inflate and deflate. Y
🤷🏻♀️ HOW? You set the trigger source. There are many options, but we'll focus on the 2 most common: EKG & pressure triggering.
23/37
Let's review the relationship b/w electrical & mechanical events
R wave: start of electrical systole, occurs JUST BEFORE mechanical systole
Middle of T wave: electrical diastole, occurs JUST BEFORE mechanical diastole
🔑: electrical stuff occurs just b4 mechanical stuff
Let's review the relationship b/w electrical & mechanical events
R wave: start of electrical systole, occurs JUST BEFORE mechanical systole
Middle of T wave: electrical diastole, occurs JUST BEFORE mechanical diastole
🔑: electrical stuff occurs just b4 mechanical stuff
24/37
⚡️ EKG TRIGGERING⚡️
EKG leads communicate with to the IABP console.
Since electrical events occur before mechanical events, the IABP has time to inflate or deflate based on the electrical events making EKG a good trigger source.
Cool, right?
⚡️ EKG TRIGGERING⚡️
EKG leads communicate with to the IABP console.
Since electrical events occur before mechanical events, the IABP has time to inflate or deflate based on the electrical events making EKG a good trigger source.
Cool, right?
25/37
There are three different EKG trigger modes
⚡️ Pattern
⚡️ Peak
⚡️ Afib
There are three different EKG trigger modes
⚡️ Pattern
⚡️ Peak
⚡️ Afib
26/37
PATTERN mode:
IABP uses the R wave of the EKG as a signal to deflate and the middle of the T to inflate.
Use this mode when you regular rhythm, HR <130, narrow QRS
PATTERN mode:
IABP uses the R wave of the EKG as a signal to deflate and the middle of the T to inflate.
Use this mode when you regular rhythm, HR <130, narrow QRS
27/37
PEAK mode:
Similar to pattern mode, also detects the R wave. To do so it finds the highest voltage and defines that as the R wave (hence the name "peak")
Can be used with a wide QRS or HR >130.
Similar to pattern mode, you still need a regular rhythm.
PEAK mode:
Similar to pattern mode, also detects the R wave. To do so it finds the highest voltage and defines that as the R wave (hence the name "peak")
Can be used with a wide QRS or HR >130.
Similar to pattern mode, you still need a regular rhythm.
28/37
👉IMPORTANT 👈
PATTERN & PEAK require a regular rhythm because the IABP determines timing based on the last few cardiac cycles (this is called training).
You do NOT get real time EKG evaluation w/ these--the IABP is expecting intervals to stay the same going forward.
👉IMPORTANT 👈
PATTERN & PEAK require a regular rhythm because the IABP determines timing based on the last few cardiac cycles (this is called training).
You do NOT get real time EKG evaluation w/ these--the IABP is expecting intervals to stay the same going forward.
29/37
Ok, cool. But what do you do if the patient has an irregular rhythm and the R-R interval is not constant? Wouldn't a wonky EKG would lead to wonky balloon inflation?
Great question. I'm glad you asked! This is when we can use afib mode.
Ok, cool. But what do you do if the patient has an irregular rhythm and the R-R interval is not constant? Wouldn't a wonky EKG would lead to wonky balloon inflation?
Great question. I'm glad you asked! This is when we can use afib mode.
30/37
AFIB mode:
Works with an irregular rhythm because you get real time analysis of the EKG (and therefore R waves).
The IABP deflates with every R wave because the machine is constantly sensing R-waves. It is not making an assumption about when the next R wave will be.
AFIB mode:
Works with an irregular rhythm because you get real time analysis of the EKG (and therefore R waves).
The IABP deflates with every R wave because the machine is constantly sensing R-waves. It is not making an assumption about when the next R wave will be.
31/37
🤔 This can be confusing.
📚 Let's quickly review EKG triggering.
Peak & pattern: IABP looks at a few beats and uses this interval going forward. It assumes the interval will stay the same. (Exact mech. differs between the 2 modes)
AFIB mode: real time EKG analysis.
🤔 This can be confusing.
📚 Let's quickly review EKG triggering.
Peak & pattern: IABP looks at a few beats and uses this interval going forward. It assumes the interval will stay the same. (Exact mech. differs between the 2 modes)
AFIB mode: real time EKG analysis.
32/37
Now, let's move on to pressure triggering
🌊PRESSURE 🌊
Uses the arterial wave form as a trigger source
Remember the waveform from the 1st tweetorial?
- Dicrotic notch = start of diastole = signal for INFLATION
- Start of upslope = start of systole = signal for DEFLATION
Now, let's move on to pressure triggering
🌊PRESSURE 🌊
Uses the arterial wave form as a trigger source
Remember the waveform from the 1st tweetorial?
- Dicrotic notch = start of diastole = signal for INFLATION
- Start of upslope = start of systole = signal for DEFLATION
33/37
For those who learn best with videos or want more details and discussion of other triggering modes, check out @KatieV_MD's Devices in a Dash youtube series. They are amazingly well done. Very strongly recommend!
For those who learn best with videos or want more details and discussion of other triggering modes, check out @KatieV_MD's Devices in a Dash youtube series. They are amazingly well done. Very strongly recommend!
34/37
Guess what? We made it to the end of part 2! This was a lot.
(I've debated the best way to split up these tweetorials--longer vs. shorter chunks. I've clearly chosen longer, but am open to suggestions!)
Guess what? We made it to the end of part 2! This was a lot.
(I've debated the best way to split up these tweetorials--longer vs. shorter chunks. I've clearly chosen longer, but am open to suggestions!)
35/37
Once again, thank you to the really stellar community @CardioNerds who helped with this tweetorial, especially @KatieV_MD & @AmitGoyalMD for their feedback.
📅 Next up in this series: cases
Once again, thank you to the really stellar community @CardioNerds who helped with this tweetorial, especially @KatieV_MD & @AmitGoyalMD for their feedback.
📅 Next up in this series: cases
36/37
References:
🎈
🎈https://t.co/kHytsuAHJv
🎈Lecture by @AndreaElliottUM from the interview trail
🎈https://t.co/JpItkzYN4u
🎈https://t.co/WKfBCn9vM7
🎈https://t.co/diYVulldim
🎈https://t.co/2qX7RiQpo5lms.getinge.training/lms/course/101…
pubmed.ncbi.nlm.nih.gov/25348545/
litfl.com/intra-aortic-b…
derangedphysiology.com/main/required-…
academic.oup.com/bjaed/article/…
References:
🎈
🎈https://t.co/kHytsuAHJv
🎈Lecture by @AndreaElliottUM from the interview trail
🎈https://t.co/JpItkzYN4u
🎈https://t.co/WKfBCn9vM7
🎈https://t.co/diYVulldim
🎈https://t.co/2qX7RiQpo5lms.getinge.training/lms/course/101…
pubmed.ncbi.nlm.nih.gov/25348545/
litfl.com/intra-aortic-b…
derangedphysiology.com/main/required-…
academic.oup.com/bjaed/article/…
37/37
🎈
🎈https://t.co/niQ1zKzeIz
🎈https://t.co/diYVulldim
🎈https://t.co/4rtSe9Joc9
🎈https://t.co/X3bb33AHHL
maryland.ccproject.com/wp-content/upl…
academic.oup.com/bjaed/article/…
teleflex.com/la/en/product-…
🎈
🎈https://t.co/niQ1zKzeIz
🎈https://t.co/diYVulldim
🎈https://t.co/4rtSe9Joc9
🎈https://t.co/X3bb33AHHL
maryland.ccproject.com/wp-content/upl…
academic.oup.com/bjaed/article/…
teleflex.com/la/en/product-…
• • •
Missing some Tweet in this thread? You can try to
force a refresh