Are you sitting on Twitter wondering why doctors are on one hand complaining about being understaffed & simultaneously incandescent with rage about mushrooming non-doctor roles? 🧵 for you.
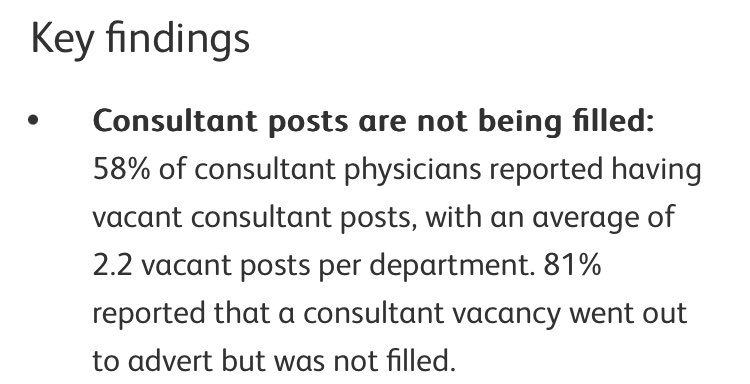
We will start off with the simple bit we can all agree on. There are not enough healthcare workers (in any part of the system, not just doctors). UK Workforce plan is clear on this and everybody agrees. …england.nhs.uk/publication/nh…
This is btw a global and not local problem which means usual developed world plan to just asset strip human resources from elsewhere is harder,
kpmg.com/xx/en/home/ins…
kpmg.com/xx/en/home/ins…
and in the UK our NHS is acquiring a solid reputation for dysfunction & poor pay. We are less competitive as a destination.
So we all agree the answer is training more staff and this includes for the medical work. This is where it gets interesting though.
Because there are broadly 3 options here. 1) Train more doctors & 2) get non-doctors to do doctors work 3) change existing doctors efficiency. 2 & 3 will be focus but 1 can be dealt with quickly.
We all agree we need more doctors… but they take ages to train. So they can’t help for at least a decade. The UK workforce plan response to this is partly to create a new 2nd class cheaper and less well trained workforce (a 🧵for another time), and
to pivot other HCWs to doctors roles. This is a rapidly evolving space- where doctors roles are being advertised (at lower pay) to nurses and AHPs.
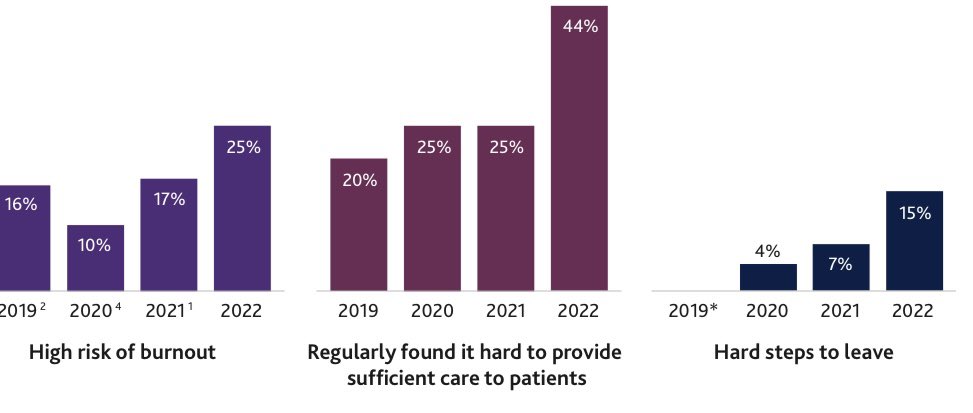
The first problem is- ask any doctor you know and they will tell you that 40% of their current job CAN AND SHOULD be done by someone else. Much of it by someone with very limited training and not a highly trained HCW. This is the crux of the issue.
Doctors right now spend a lot of their time on menial administration. It’s one of the reasons they cite for burnout and stress. This is mostly the fault of 1) terrible electronic systems & 2) woeful underinvestment in admin support.
Doctor’s efficiency could be dramatically increased by reinvesting in admin both in hospitals broadly & in support of doctors specifically. Doesn’t require much training other than on the job and they are not expensive to employ.
A rapid expansion of physicians assistant, doctors secretaries, admin support for units etc would instantly improve doctors efficiency. Longer term we need a laser-like and co-ordinated approach to improving IT but short term why is nobody even talking about this?
I’ll pop on my tinfoil hat in a second but before I do the other reason repurposing nurses and APHs to do highly skilled medical roles will not work, even in short term, and it is nose-plain-face obvious. We don’t have enough of them to do even their current roles.
There is just as much (and arguably more) of a crisis in the rest of HCW job market. This solves nothing. So why propose it as a major solution?
Down the rabbit hole. Doctors used to be unequivocal decision-makers in healthcare system. That has been intentionally dismantled over 2 decades. We are completely marginalised now in major decisions & it is 💯 the intention of both current govt & employers to press advantage
by further de-professionalising medicine, introducing a cheaper, more easily manipulated alternate workforce. Employing a raft of support staff would be both an acknowledgement of our importance & a consolidation of our agency.
Basically employers/govt would be saying- we know what you do is important and not replaceable so here are extra resources to help you do it.
I am completely behind the need to dramatically change many things about working life and practice in healthcare. I am a true believer in specialist roles.
My own specialist service is ‘specialist’ because of them. I am however completely against the current & mendacious orchestrated attempt to undermine doctors & disempower them. We need clear leadership to push against it.
• • •
Missing some Tweet in this thread? You can try to
force a refresh