
37 degrees Celsius, 98.6 Fahrenheit. That's normal body temperature, right?
Wrong.
New data suggests true "normal" is 98.0 degrees. (thread)
Wrong.
New data suggests true "normal" is 98.0 degrees. (thread)
We get 98.6 degrees from this guy Karl Wunderlich, who measured 1,000,000 temperatures from 25,000 Germans in the mid 1800s. He was really the first to realize that "fever" was not itself a disease, but a symptom of a disease. 

He took the average, got 98.6, and that was that. UNTIL NOW.
(Ok honestly, people have known this was wrong for a while, but the new data is cool).
From @JAMAInternalMed:
(Ok honestly, people have known this was wrong for a while, but the new data is cool).
From @JAMAInternalMed:
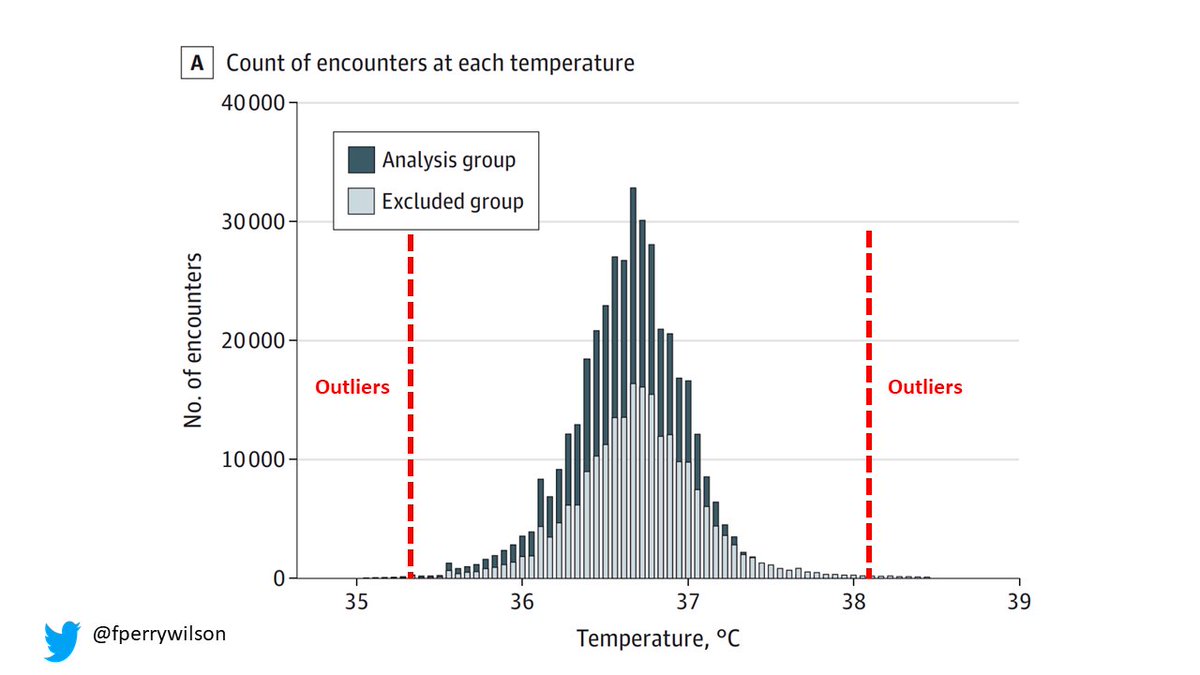
Thanks to the electronic health record, we have access to countless temperatures taken during clinical visits. Can we just average those?

Of course not. People see their docs for reasons, and some of those reasons cause fever. Before the new paper, people estimating normal would just exclude people with diagnosis codes associated with fever (infections, etc).
But that's sort of arbitrary. What the authors do here is use an algorithm called LIMIT that identifies diagnosis codes disproportionately present in the tails of distribution. Not arbitrary at all.
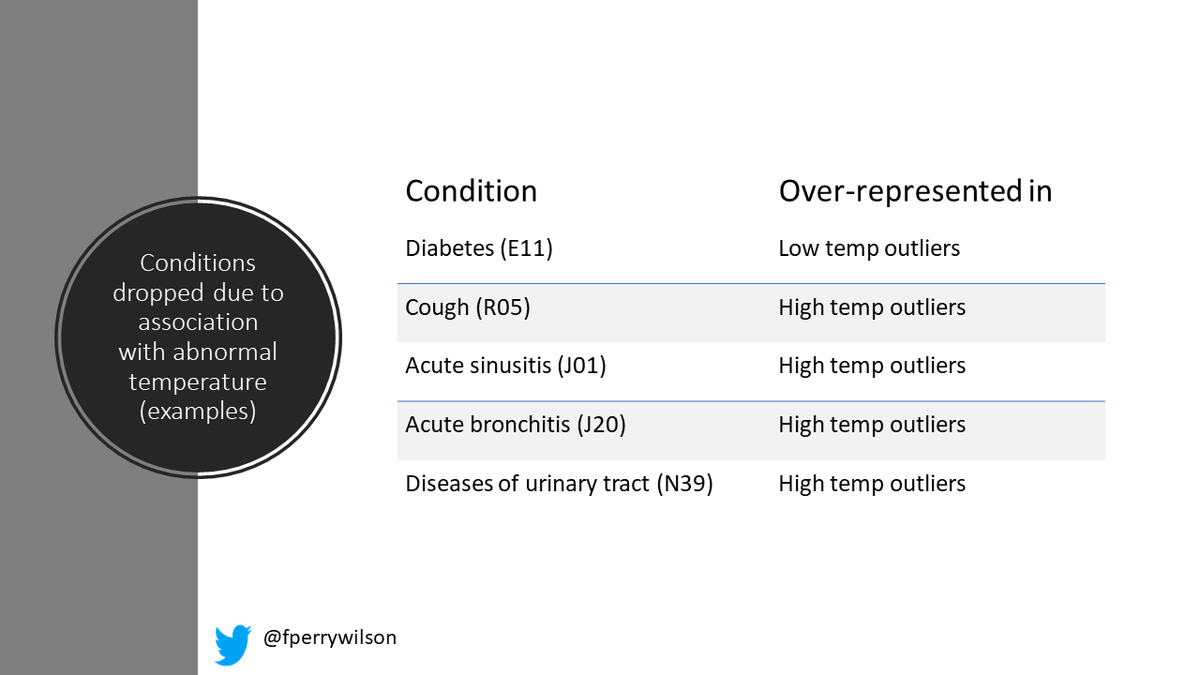
That's a data-driven way to find a diagnosis that does something to body temperature. And a lot of these were predictable (cough, UTI), but actually diabetes was MUCH more prevalent in the low outliers body temp-wise. So ALL people with diabetes were dropped from the "normal" pop
Once you drop all people with codes that, according to the data, might affect temperature, you can (finally) take the mean. And you get...
36.6 C, 98.0 F.
36.6 C, 98.0 F.
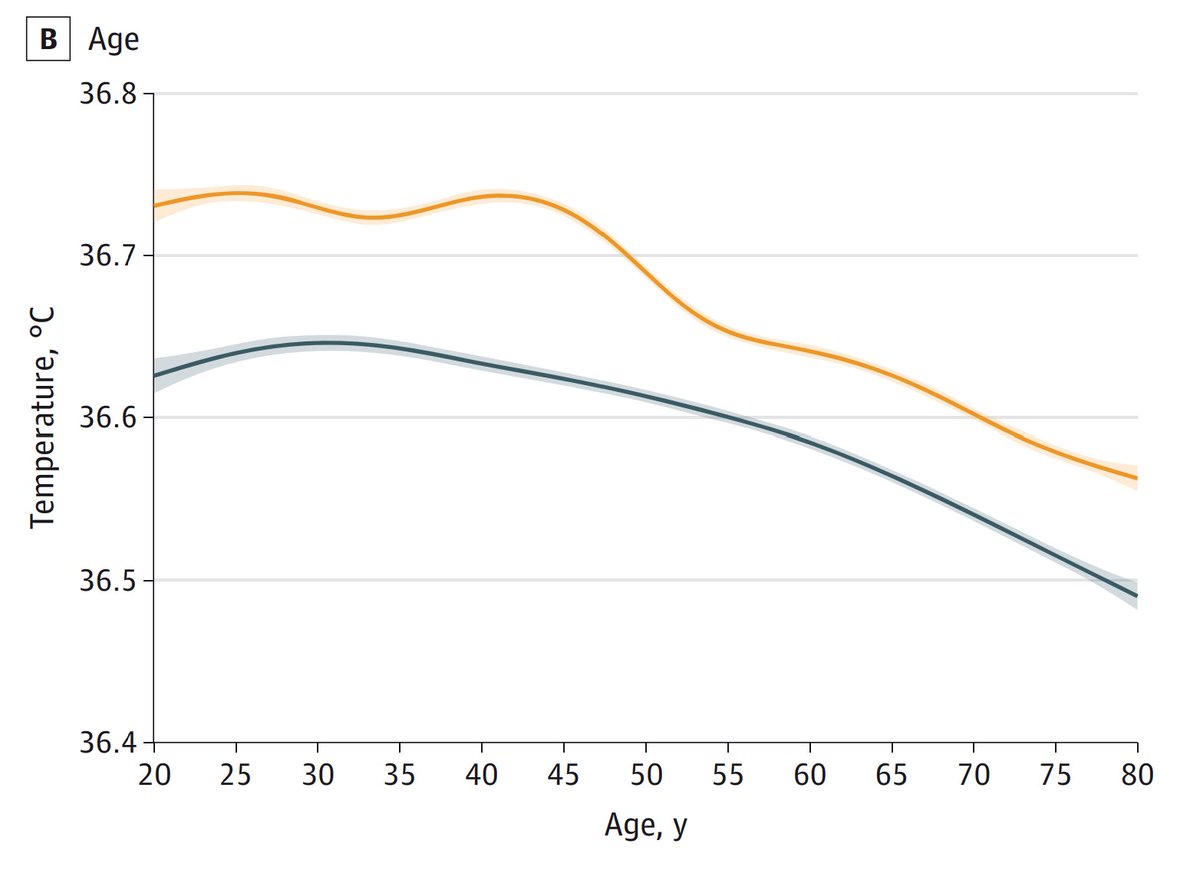
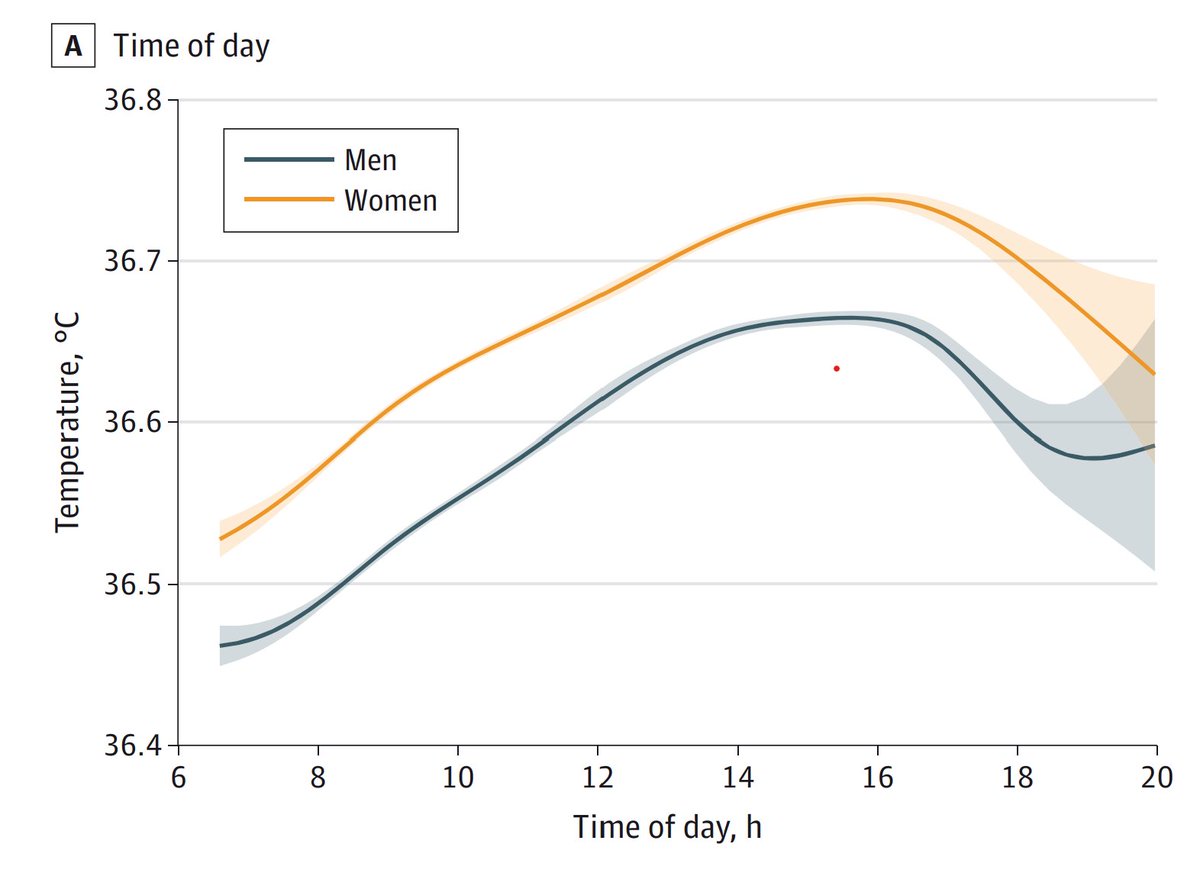
Of course, this varies by age, sex, and time of day as you can see here.
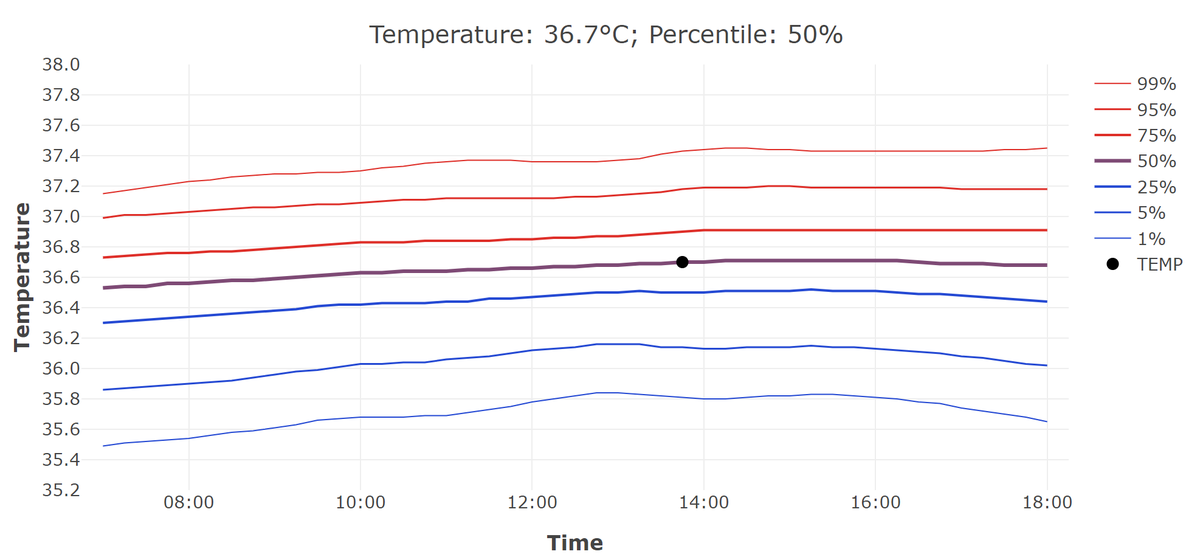
They even created a little web calculator that you can visit which will tell you YOUR normal temperature based on these parameters. Here's mine for 2pm.
normaltemperature.stanford.edu
normaltemperature.stanford.edu
So, yup, humans are colder-blooded than we thought. And now (for once) Fahrenheit gets the nice round number. Sorry metric bros.
More detail in my column on @medscape here. medscape.com/viewarticle/99…
More detail in my column on @medscape here. medscape.com/viewarticle/99…
• • •
Missing some Tweet in this thread? You can try to
force a refresh













