Gadolinium in dialysis patients.
What's up with that?
#Tweetorial
1/11
What's up with that?
#Tweetorial
1/11
Nephrogenic systemic fibrosis (NSF) is an iatrogenic disease that presents with hardening of the skin and other organs. It is often lethal. I treated 5 people with this condition (including one with AKI). Terrible.
2/11
2/11

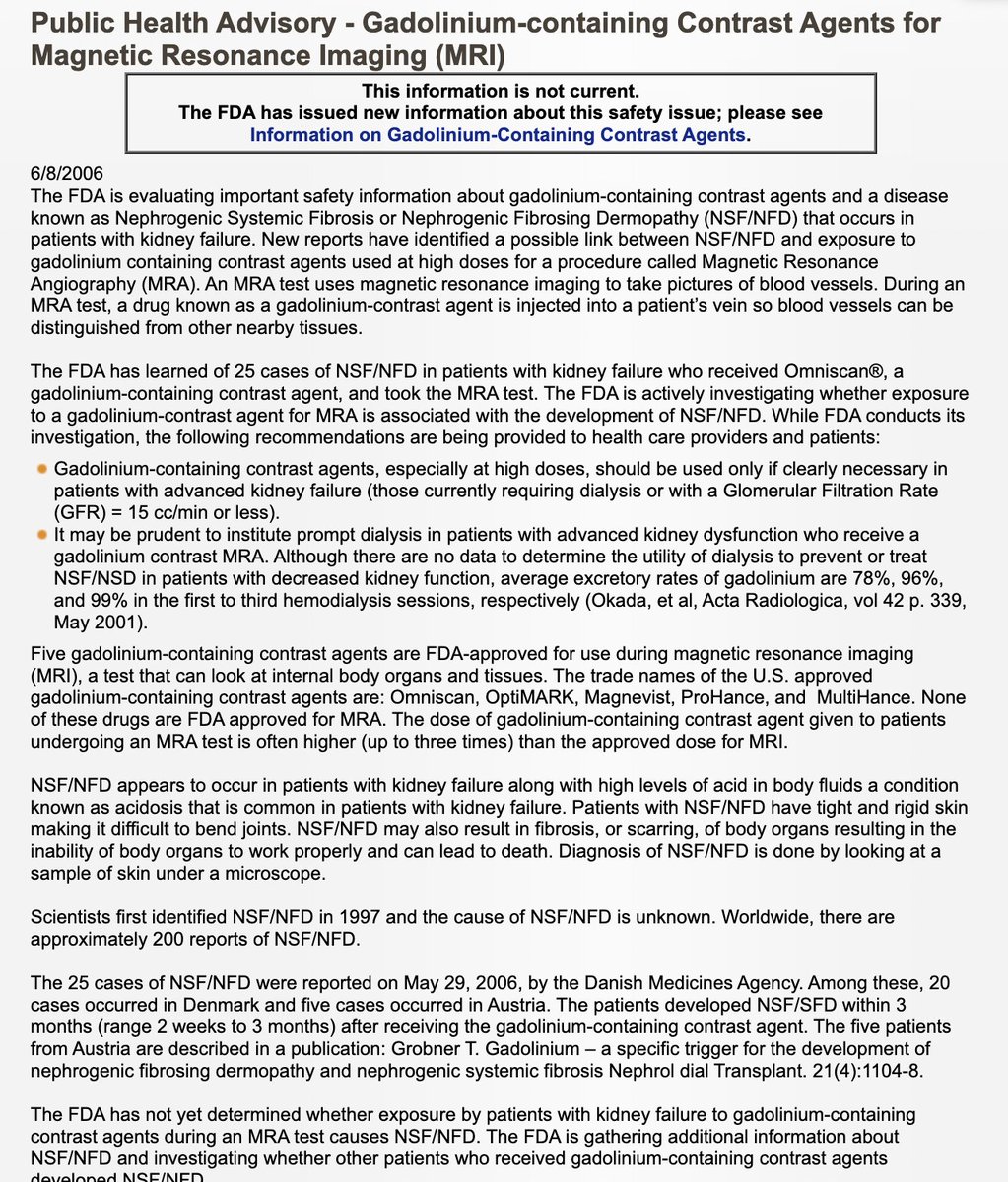
The etiology of NSF was unknown and there were many theories. In 2006, Thomas Grobner published a small case series showing 5 patients developing NSF within weeks of receiving gadolinium contrast for MRI.
3/11pubmed.ncbi.nlm.nih.gov/16431890/
3/11pubmed.ncbi.nlm.nih.gov/16431890/
This observation and theory was rapidly replicated and accepted as the cause of NSF. Nephrologists and radiologists stopped giving gadolinium to patients on dialysis and I haven't seen a case since.
4/11
4/11
In 2006 the FDA warned physicians and the public about the risk and then in 2007 added black box warnings to gadolinium based contrast agent package labels.
5/11 wayback.archive-it.org/7993/201610222…
5/11 wayback.archive-it.org/7993/201610222…
But as we looked at the data further it appeared that not all contrast agents had the same toxicity. Gadodiamide (OmniScan) was the agent in 90% of the cases despite having a market share of only 30%.
6/11 ncbi.nlm.nih.gov/pmc/articles/P…
6/11 ncbi.nlm.nih.gov/pmc/articles/P…

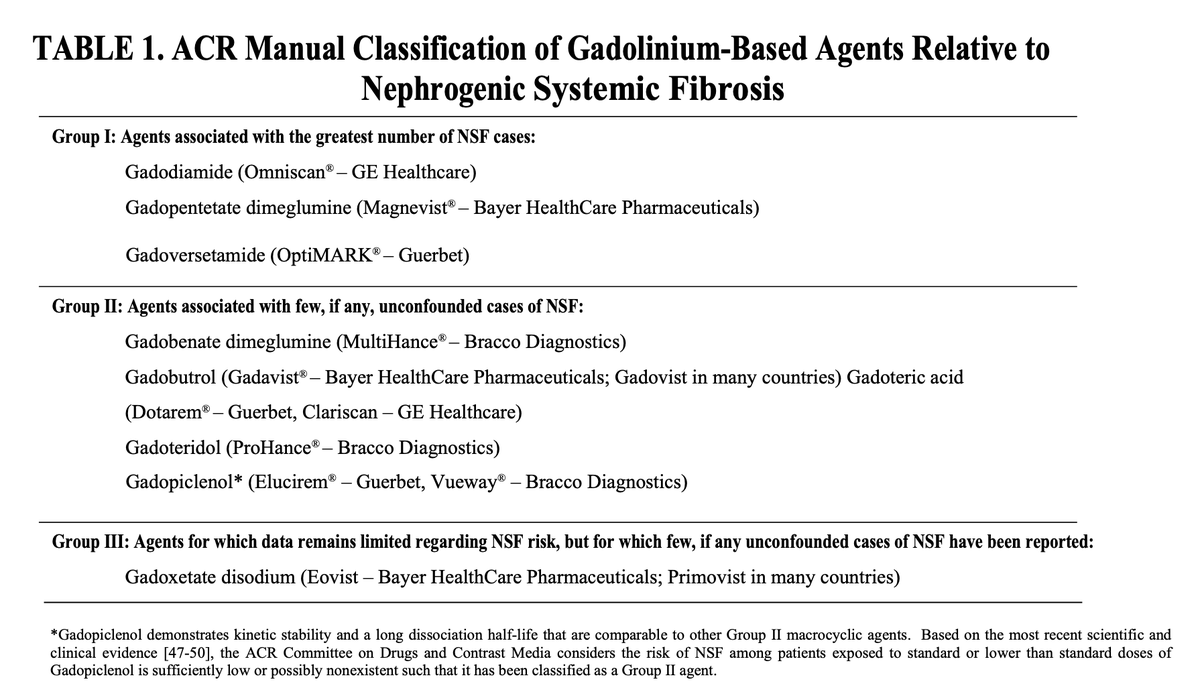
The American College of Radiology (ACR) breaks down gadolinium based contrast agents (GBCA) into three categories based on the risk of NSF with:
Group 1 being high risk
Group 2 being low risk
Group 3 being unknown
7/11
Group 1 being high risk
Group 2 being low risk
Group 3 being unknown
7/11
The obvious recommendation is to choose GBCA from Group 2 and this was backed up by a meta analysis showing that following 4931 administrations of Group 2 GBCA to patients with CKD stage 4, 5 and ESRD, there were ZERO cases of NSF!
8/11 jamanetwork.com/journals/jamai…
8/11 jamanetwork.com/journals/jamai…

For a deep dive into this check out @NephJC's coverage of this meta analysis:
or listen to the @FreelyFiltered podcast on the same manuscript
9/11nephjc.com/news/gad-not-s…
nephjc.com/freelyfiltered…
or listen to the @FreelyFiltered podcast on the same manuscript
9/11nephjc.com/news/gad-not-s…
nephjc.com/freelyfiltered…
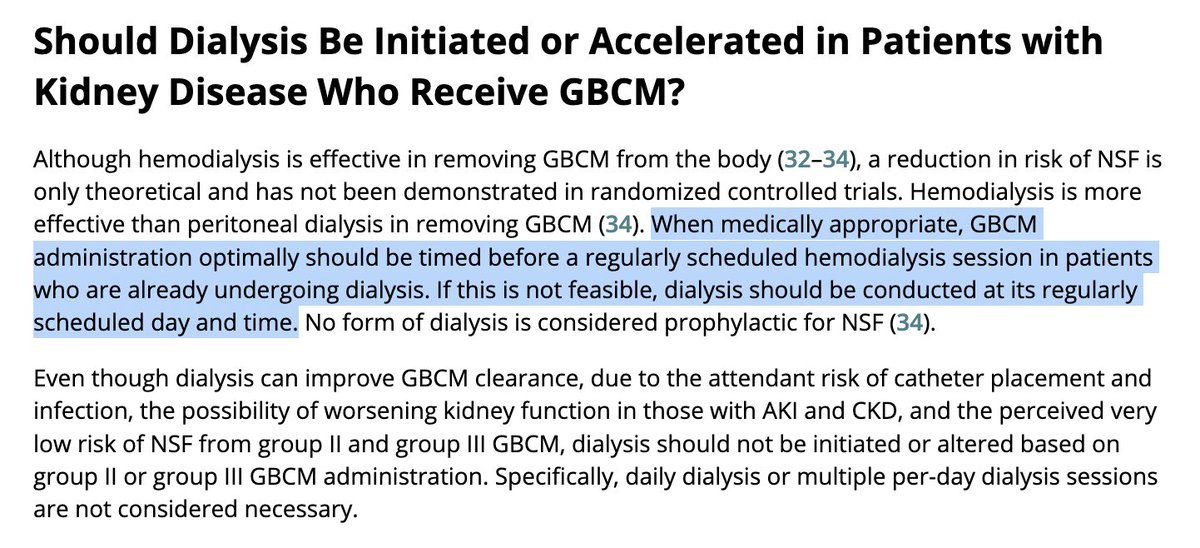
Gadolinium is removed by dialysis, with approximately 65% removed with a single dialysis session, and the ACR recommends dialyzing people after gad administration but not to initiate dialysis in patients with advanced CKD not on dialysis.
10/11 pubs.rsna.org/doi/full/10.11…
10/11 pubs.rsna.org/doi/full/10.11…
How is gad in ESRD handled at your institution
11/11
11/11
@BurgersAreYummy @ebtapper pubmed.ncbi.nlm.nih.gov/9653466/
• • •
Missing some Tweet in this thread? You can try to
force a refresh