
🚀Na over-correction (Na📈) as THE (only) cause of ODS/CPM: An absurd over-simplification.
Since 1980s, Na📈 has been portrayed as the main cause of CPM (so far as now the terms ODS and CPM are used synonymously).
However, finding the truth (if it exists) is more complicated.
🧵..
1/
Since 1980s, Na📈 has been portrayed as the main cause of CPM (so far as now the terms ODS and CPM are used synonymously).
However, finding the truth (if it exists) is more complicated.
🧵..
1/
1959 saw the very first report of CPM in literature by Adams
Prominent words = ‘Alcoholic’ & ‘Malnourished’
In these 4 cases, 2 had Na<120 (per later report). Na📈 unknown.
2/
Prominent words = ‘Alcoholic’ & ‘Malnourished’
In these 4 cases, 2 had Na<120 (per later report). Na📈 unknown.
2/
Let’s move to 1967
McCormick consolidates 69 cases of CPM
Malnutrition (77%)
Alcoholics (50%)
Baseline neurological disease (20%)
Na not explicitly mentioned but ‘severe electrolyte abnormalities’ is (in 33%).
3/
McCormick consolidates 69 cases of CPM
Malnutrition (77%)
Alcoholics (50%)
Baseline neurological disease (20%)
Na not explicitly mentioned but ‘severe electrolyte abnormalities’ is (in 33%).
3/
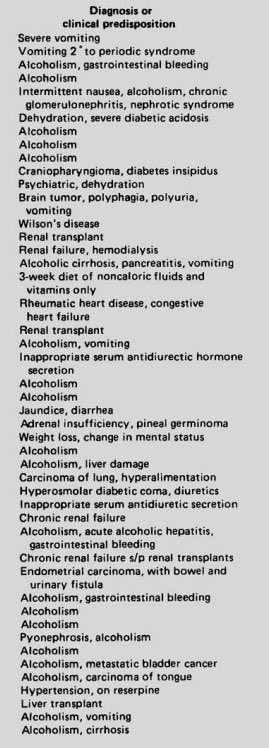
Then came many case reports & the 1977 paper by Bucar noting hypoNa as a possible risk factor.
Review of 46 cases:
~25% with Na<120
Look at their dx list:
4/
Review of 46 cases:
~25% with Na<120
Look at their dx list:
4/
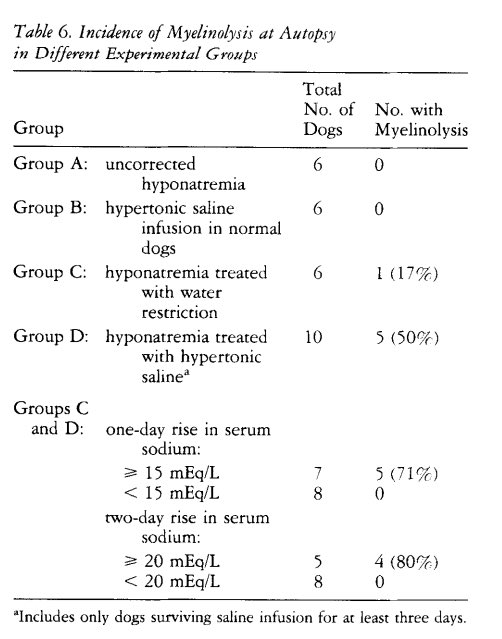
Then came the two animal studies associating Na📈 with CPM:
High chances of CPM with 24 hour Na📈 of:
15 or 20 (dogs)
12 (rats)
5/
High chances of CPM with 24 hour Na📈 of:
15 or 20 (dogs)
12 (rats)
5/
Corroborated by human studies:
Initial data was scary - ODS incidence was attributed at 15-25% in severe hypoNa
By the early 1990s, ODS (now an established term) is mainly attributed to Na📈
6/
Initial data was scary - ODS incidence was attributed at 15-25% in severe hypoNa
By the early 1990s, ODS (now an established term) is mainly attributed to Na📈
6/
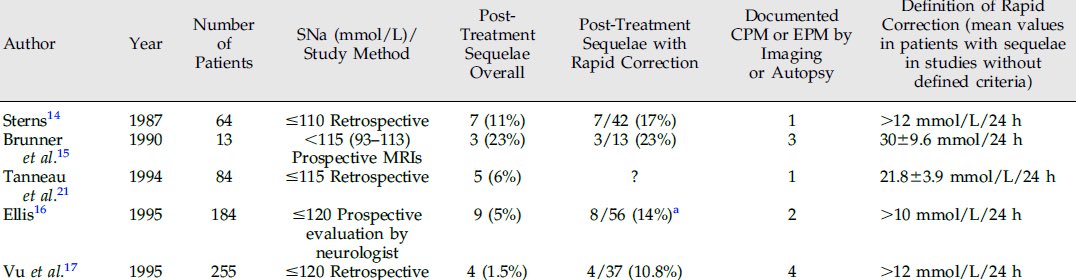
Changing the goalposts:
Notice above how so few cases have CPM by imaging/autopsy?
Thats the big change from before: Separation of ODS and CPM
In rapid correctors, neurological findings without supporting imaging/autopsy were characterized as ‘clinical’ ODS.
The ‘expert opinion’ was that ODS Dx did not require supportive imaging findings (aka central or extra pontine myelinolysis)
7/
Notice above how so few cases have CPM by imaging/autopsy?
Thats the big change from before: Separation of ODS and CPM
In rapid correctors, neurological findings without supporting imaging/autopsy were characterized as ‘clinical’ ODS.
The ‘expert opinion’ was that ODS Dx did not require supportive imaging findings (aka central or extra pontine myelinolysis)
7/
By this time (1990s), emphasis was predominantly on Na 📈 and risk factors like alcoholism, malnutrition etc. became footnotes.
Next 20 years - guidelines for Na 📈 became more and more strict.
Goal: Prevention of ODS
A Dx characterized as devastating:
-With high mortality (not true)
-Requiring no imaging findings
-Can occur weeks to months after Na 📈
-(Almost) Totally preventable by slow Na 📈
8/
Next 20 years - guidelines for Na 📈 became more and more strict.
Goal: Prevention of ODS
A Dx characterized as devastating:
-With high mortality (not true)
-Requiring no imaging findings
-Can occur weeks to months after Na 📈
-(Almost) Totally preventable by slow Na 📈
8/
Which led to the bad part 👇
Practice changes that happened as a result of this:
-Every single hypoNa patient is treated according to these limits without any differentiation of risk factors or clinical status or many times even starting Na.
-Bigtime hesitancy in using 3% saline (only used in 12% of our cohort in the first 24 hours)
-Huge time/effort spent bringing Na down in any patient when correction limits are exceeded
-Days and days of languishing at low Na increasing hospital stay & additional risk that comes with it
9/
Practice changes that happened as a result of this:
-Every single hypoNa patient is treated according to these limits without any differentiation of risk factors or clinical status or many times even starting Na.
-Bigtime hesitancy in using 3% saline (only used in 12% of our cohort in the first 24 hours)
-Huge time/effort spent bringing Na down in any patient when correction limits are exceeded
-Days and days of languishing at low Na increasing hospital stay & additional risk that comes with it
9/
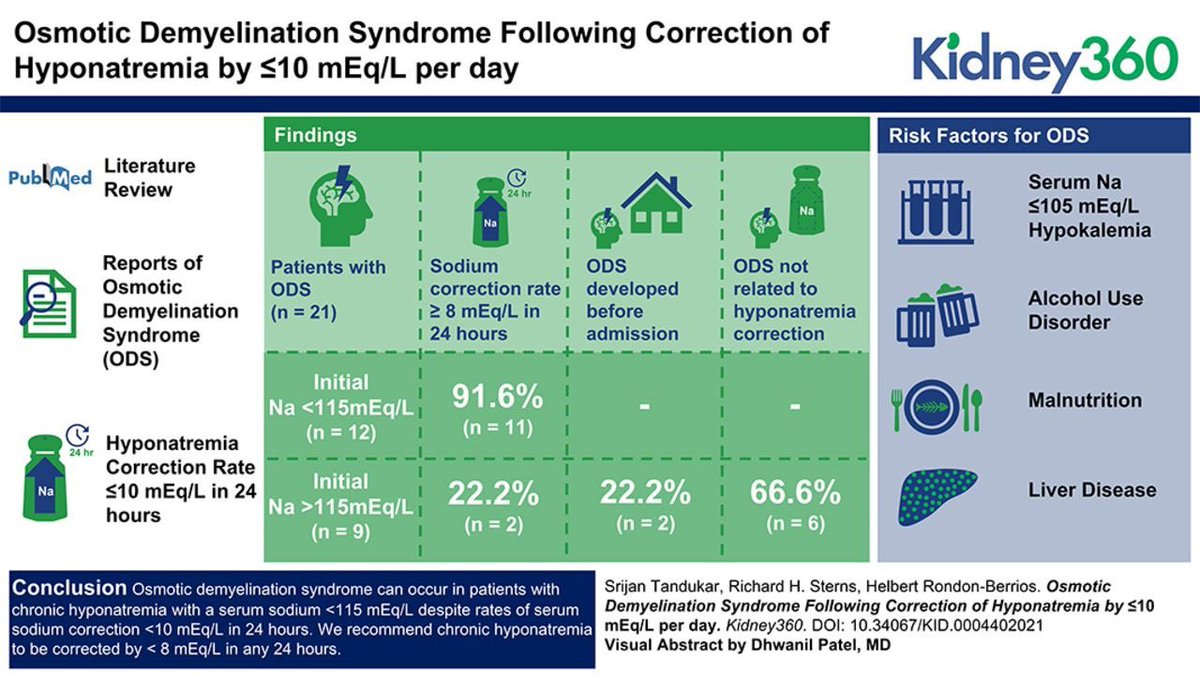
Over the years:
Many case reports of ODS occurring despite slow/meticulous Na 📈
Some consolidated in this one below. Author conclusion: CPM occurs if Na 📈<10, so <8 should be the goal. 🤦🏼♂️
10/
Many case reports of ODS occurring despite slow/meticulous Na 📈
Some consolidated in this one below. Author conclusion: CPM occurs if Na 📈<10, so <8 should be the goal. 🤦🏼♂️
10/
Now:
MacMillan et al:
22,858 hosp, Na<130 → 12 w ODS (7 with Na 📈 ≤8)
Our paper:
3274 pts, Na<120 → 7 w ODS (5 with Na 📈 ≤8).
Outcome: only 1 patient did not fully recover - gait abnormalities [no data in 1 other pt]
11/
MacMillan et al:
22,858 hosp, Na<130 → 12 w ODS (7 with Na 📈 ≤8)
Our paper:
3274 pts, Na<120 → 7 w ODS (5 with Na 📈 ≤8).
Outcome: only 1 patient did not fully recover - gait abnormalities [no data in 1 other pt]
11/
ODS is rare (much rarer than previously claimed) but what about CPM on Imaging? Turns out it’s much more common outside the narrow hypoNa (nephrology) world:
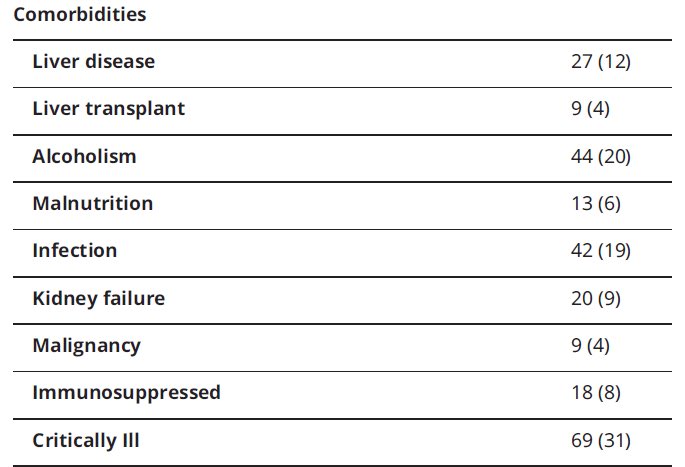
Neurology study of all CPM cases in our centers x 20 years:
45 cases, >75% had Na>130
Look at the risk factors: Alcoholism, Liver disease, Critical illness etc.
Here in lies the issue:
Many of these high risk pts
*may have CPM without/unrelated to Na or if hyponatremic, even before Na 📈
*have high burden of waxing & waning neurological symptoms unrelated to Na levels
12/
Neurology study of all CPM cases in our centers x 20 years:
45 cases, >75% had Na>130
Look at the risk factors: Alcoholism, Liver disease, Critical illness etc.
Here in lies the issue:
Many of these high risk pts
*may have CPM without/unrelated to Na or if hyponatremic, even before Na 📈
*have high burden of waxing & waning neurological symptoms unrelated to Na levels
12/
Summary:
✅CPM has many risk factors other than Na 📈
✅CPM predominantly occurs in non-hyponatremic settings
✅Na 📈 is the straw that breaks the camel’s back & recent evidence does not back up claims that 6 or 8/24h is safe.
✅High risk pts (Alcoholism/malnutrition etc.) → any speed of Na 📈 correction carries risk
Weak to No Evidence:
⛔️Clinical ODS (no CPM on imaging)
⛔️Linking CPM to Na 📈 from months ago
⛔️Re-lowering serum Na when limits are exceeded
✅CPM has many risk factors other than Na 📈
✅CPM predominantly occurs in non-hyponatremic settings
✅Na 📈 is the straw that breaks the camel’s back & recent evidence does not back up claims that 6 or 8/24h is safe.
✅High risk pts (Alcoholism/malnutrition etc.) → any speed of Na 📈 correction carries risk
Weak to No Evidence:
⛔️Clinical ODS (no CPM on imaging)
⛔️Linking CPM to Na 📈 from months ago
⛔️Re-lowering serum Na when limits are exceeded
• • •
Missing some Tweet in this thread? You can try to
force a refresh



