1/7
NAME THAT CBC
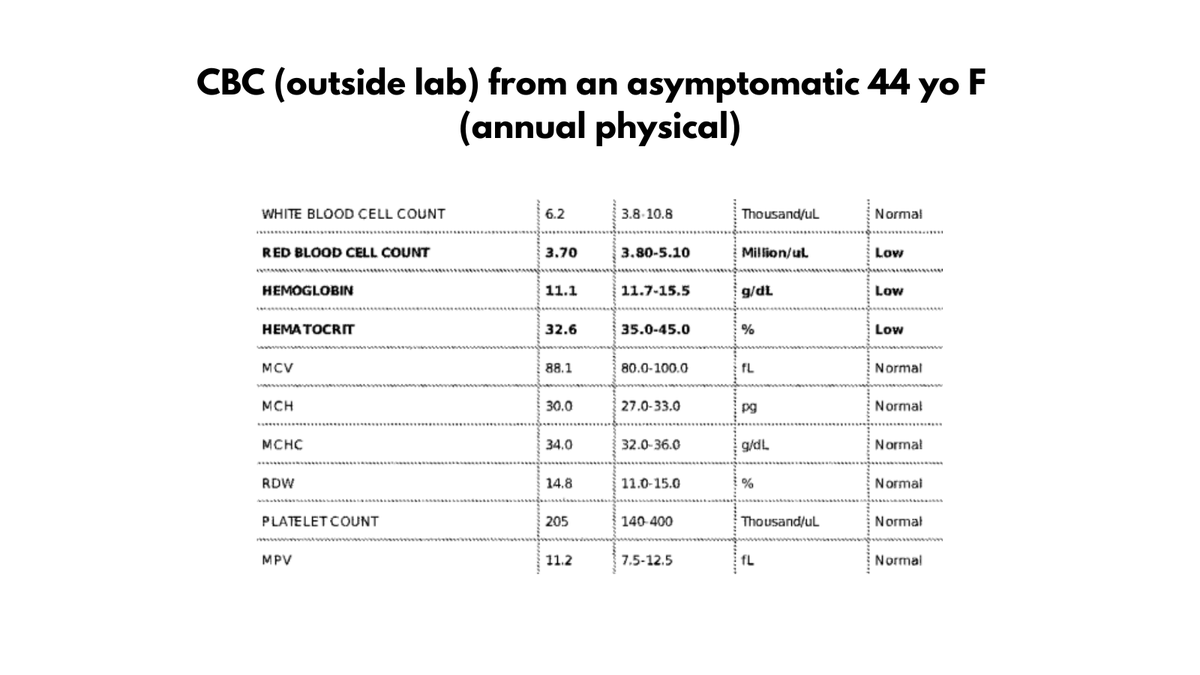
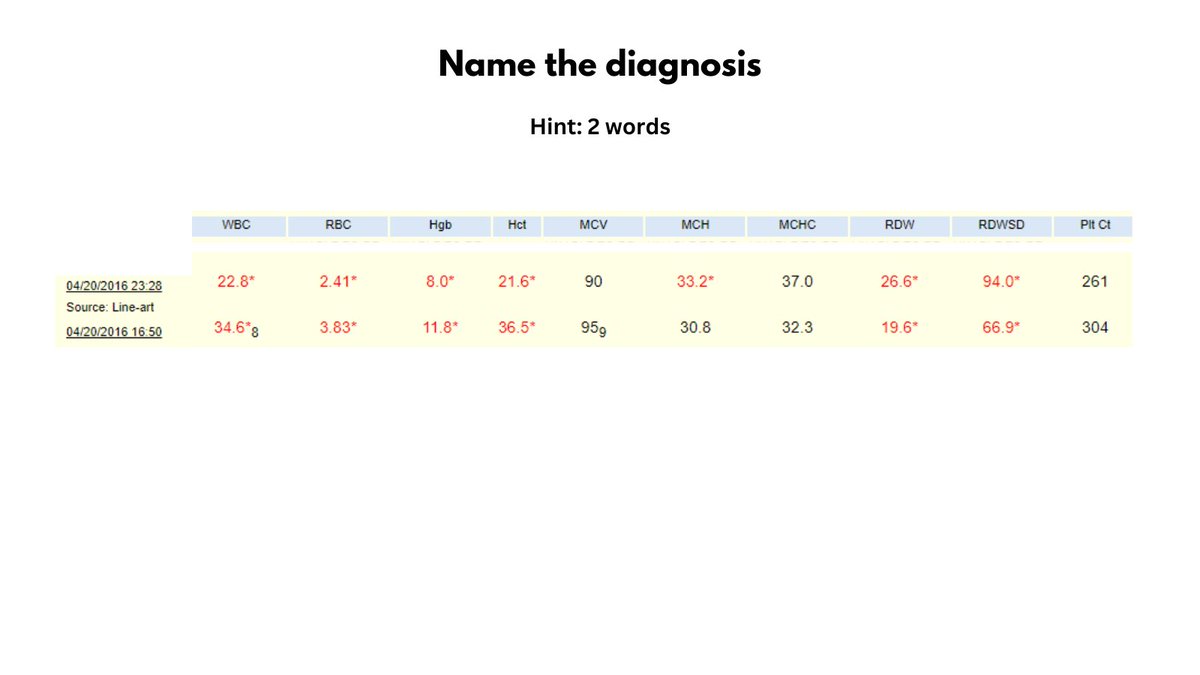
I tweeted a pair of CBCs earlier today and asked for a diagnosis in two words.
Lots of great responses!!
Kudos to @AaronBoothby2 for getting the right answer:
CLOSTRIDIAL SEPSIS
In this thread we will systematically work through the case.
NAME THAT CBC
I tweeted a pair of CBCs earlier today and asked for a diagnosis in two words.
Lots of great responses!!
Kudos to @AaronBoothby2 for getting the right answer:
CLOSTRIDIAL SEPSIS
In this thread we will systematically work through the case.
2/7
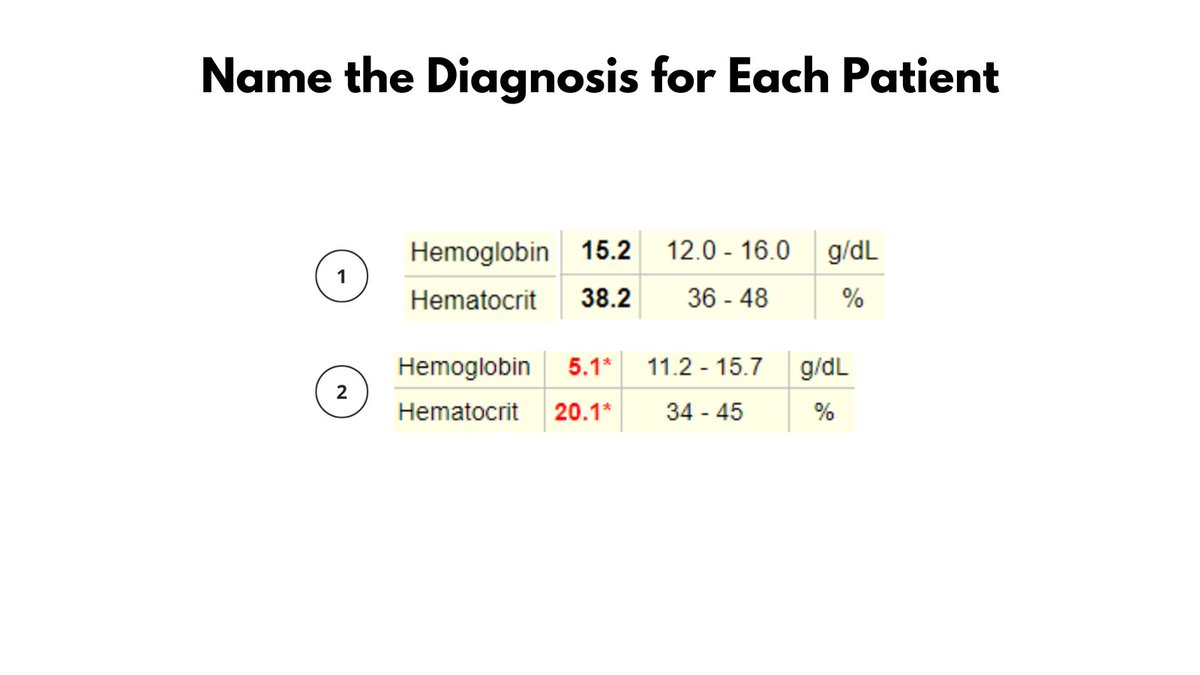
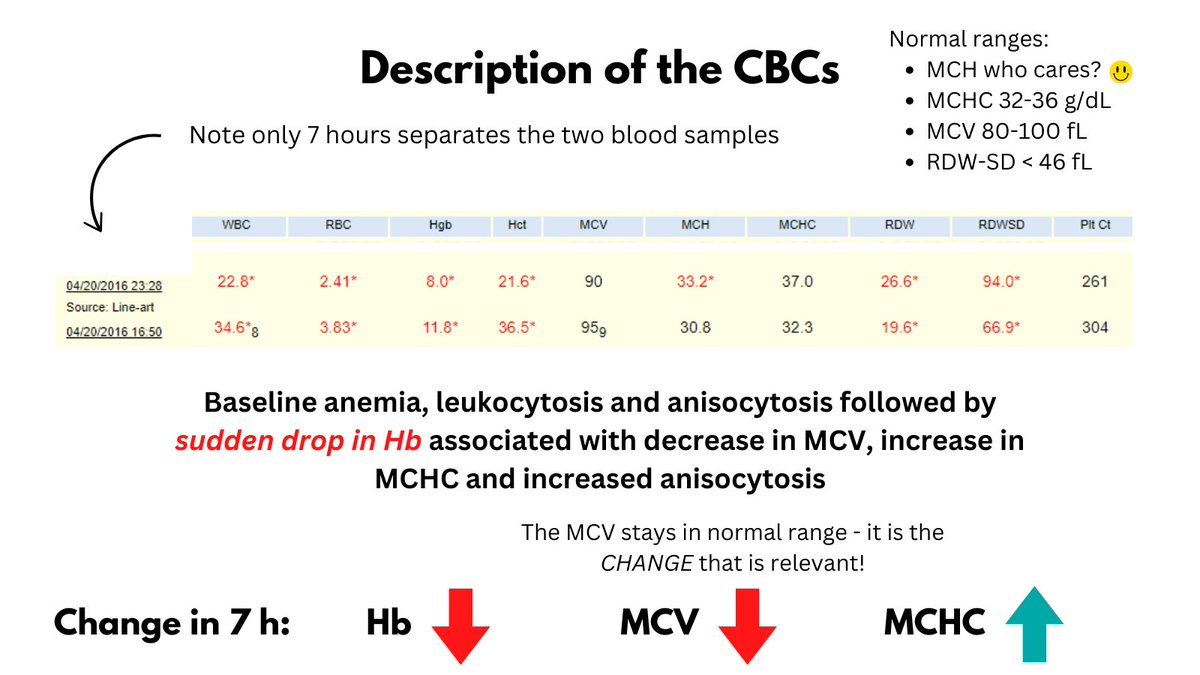
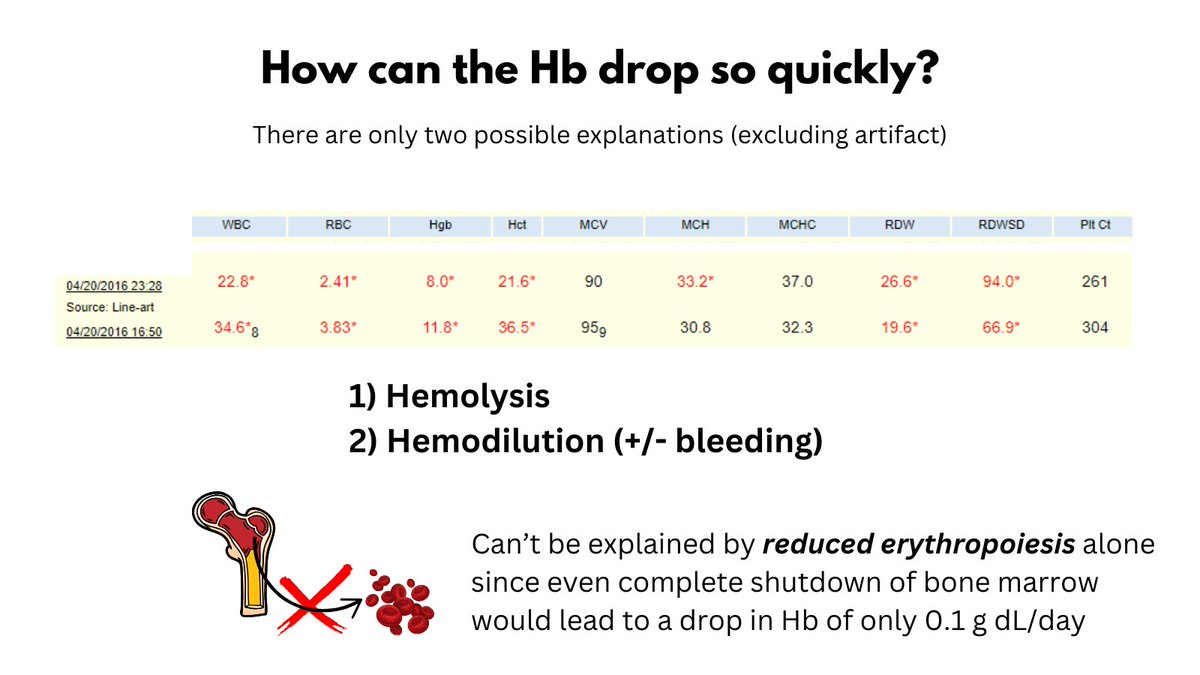
1. The first thing to note is that the two CBCs were taken a mere 7 h apart. Many notable changes occurred during this short time span, including a sudden drop in Hb and MCV and an increase in MCHC and RDW.
... it is the CHANGES in values that are meaningful.
1. The first thing to note is that the two CBCs were taken a mere 7 h apart. Many notable changes occurred during this short time span, including a sudden drop in Hb and MCV and an increase in MCHC and RDW.
... it is the CHANGES in values that are meaningful.
3/7
2. How can we explain such a rapid drop in Hb? Certainly not by a production problem. If I completely shut off my bone marrow production of RBCs, my Hb will only drop by 0.1 g/dL/day because of the long survival time of RBCs.
So, this must be hemolysis or hemodilution.
2. How can we explain such a rapid drop in Hb? Certainly not by a production problem. If I completely shut off my bone marrow production of RBCs, my Hb will only drop by 0.1 g/dL/day because of the long survival time of RBCs.
So, this must be hemolysis or hemodilution.
4/7
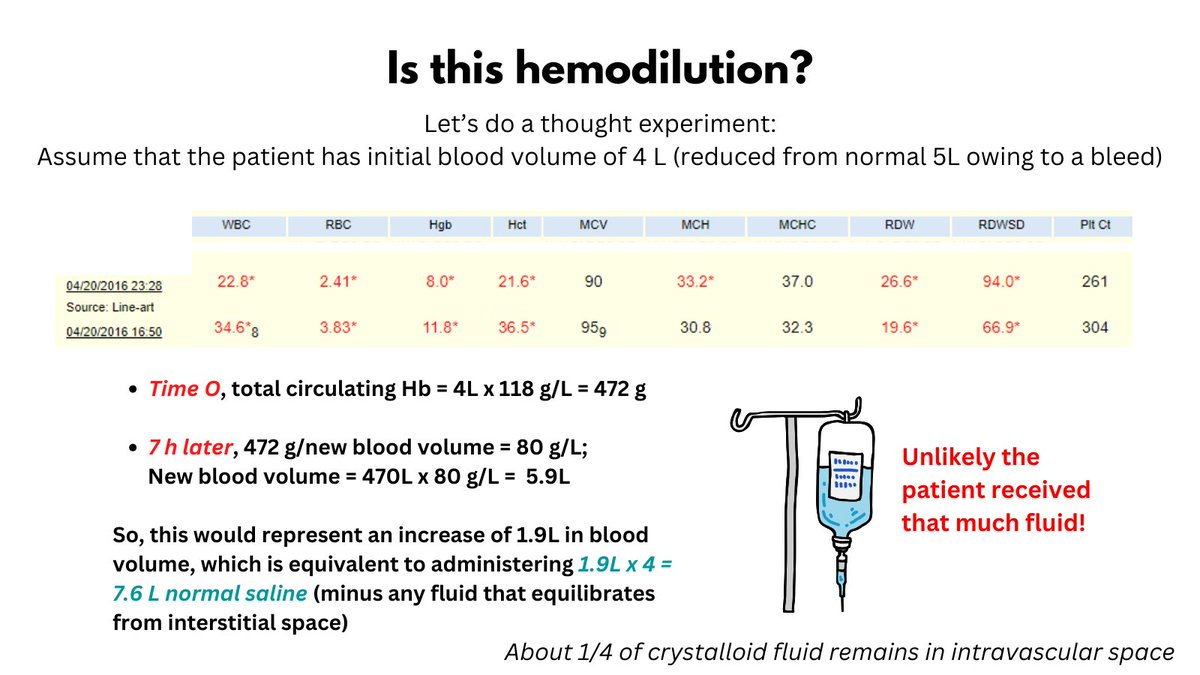
3. Let's consider hemodilution first (which would most likely occur in the context of a bleed). If we work through the numbers we find that the patient would have had to receive a ridiculous quantity of fluid to explain this degree of drop in Hb.
3. Let's consider hemodilution first (which would most likely occur in the context of a bleed). If we work through the numbers we find that the patient would have had to receive a ridiculous quantity of fluid to explain this degree of drop in Hb.
5/7
4. That leaves hemolysis as the most likely cause of the reduction in Hb. The ddx of hemolysis includes immune and non-immune causes (extracorpuscular and intracorpuscular).
4. That leaves hemolysis as the most likely cause of the reduction in Hb. The ddx of hemolysis includes immune and non-immune causes (extracorpuscular and intracorpuscular).

6/7
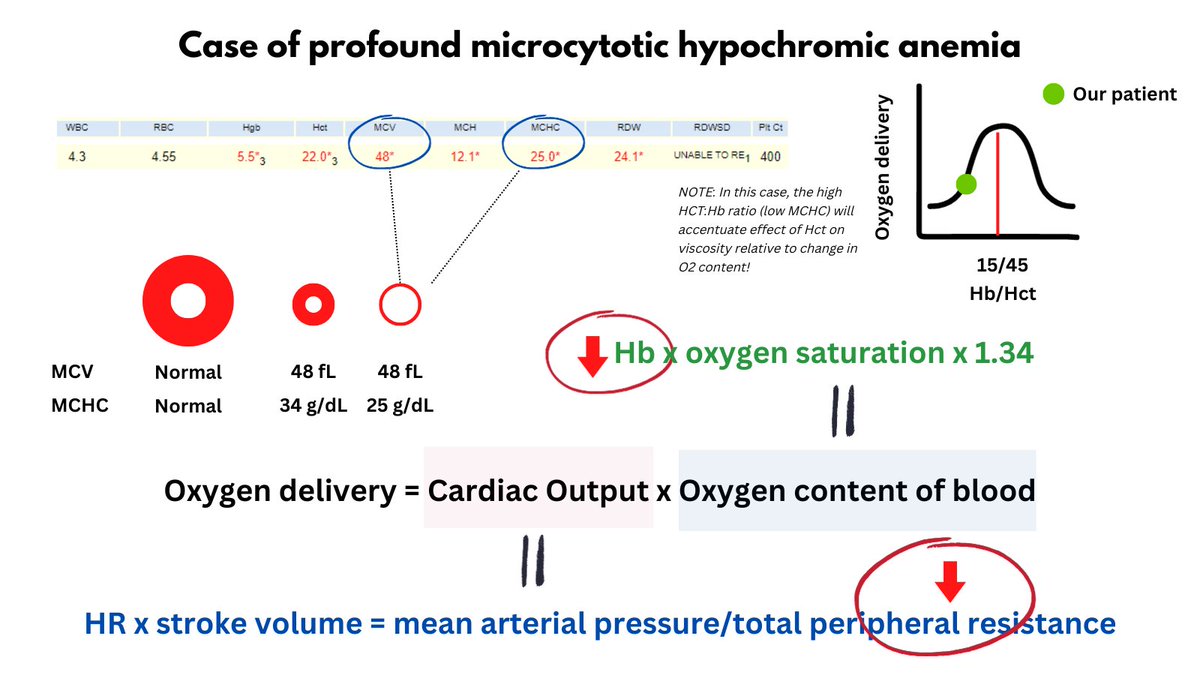
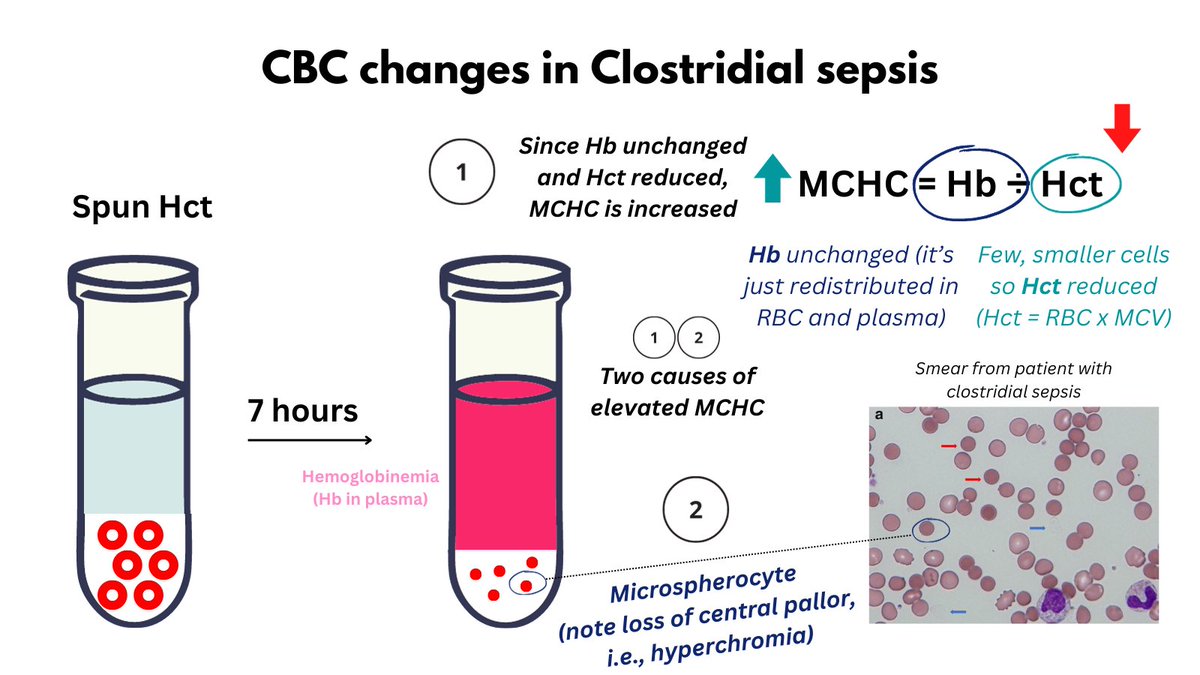
5. Considering causes of HA that are associated with elevated MCHC, the ddx narrows to AIHA (real), CAD (artifact) and infection with clostridial perfringens (real).
5. Considering causes of HA that are associated with elevated MCHC, the ddx narrows to AIHA (real), CAD (artifact) and infection with clostridial perfringens (real).
6/7
6. The MCV in CAD is artificially elevated, whereas this patient's MCV actually decreased (albeit within the normal range). The latter result is c/w AIHA or clostridium sepsis (especially the latter owing to microspherocytes).
6. The MCV in CAD is artificially elevated, whereas this patient's MCV actually decreased (albeit within the normal range). The latter result is c/w AIHA or clostridium sepsis (especially the latter owing to microspherocytes).
7/7
7. It would very unusual for a warm antibody to result in such rapid hemolysis. Moreover, the leukocytosis is a hint that there may be an underlying infection.
In fact this patient had fulminant clostridial sepsis (including classical microspherocytes on his blood smear).
7. It would very unusual for a warm antibody to result in such rapid hemolysis. Moreover, the leukocytosis is a hint that there may be an underlying infection.
In fact this patient had fulminant clostridial sepsis (including classical microspherocytes on his blood smear).
• • •
Missing some Tweet in this thread? You can try to
force a refresh