Tomorrow, a crucial piece of legislation around healthcare will be scrutinised by MPs.
It will happen in a committee room, away from the main chambers, on a whisper.
If it passes, it will worsen the health of the UK population.
Did you know about it? No?
A thread 🧵
It will happen in a committee room, away from the main chambers, on a whisper.
If it passes, it will worsen the health of the UK population.
Did you know about it? No?
A thread 🧵
Physician Associates and Anaesthesia Associates are a relatively new role, which the Government is relying on to meet the aims of the Long Term Workforce Plan. Together, along with a smaller separate surgical role, they form a group called Medical Allied Professionals (MAPs). 
They usually undergo about 2 years of training following a previous degree, unlike doctors who do at 5-6 years (sometimes 4 years with a previous degree). There are edge cases here but this is predominantly the case.
A first year doctor in the NHS works under a tight framework, so much so that they cannot fully register with the GMC for another year. To become trained to expert level, you would work for at least 5 further years to be a new GP or double that for a specialist in hospital.
A PA or AA undergoes relatively high levels of supervision for about 12-24 months, but then usually becomes autonomous. With the caveat that they must always be overseen, even if indirectly, by a senior doctor.
Further, doctor is regulated with the General Medical Council, meaning that a rogue doctor who acts well outside their scope of practice and causes harm could be held to account. They could be deregistered at a legal hearing, in a purpose that protects the public.
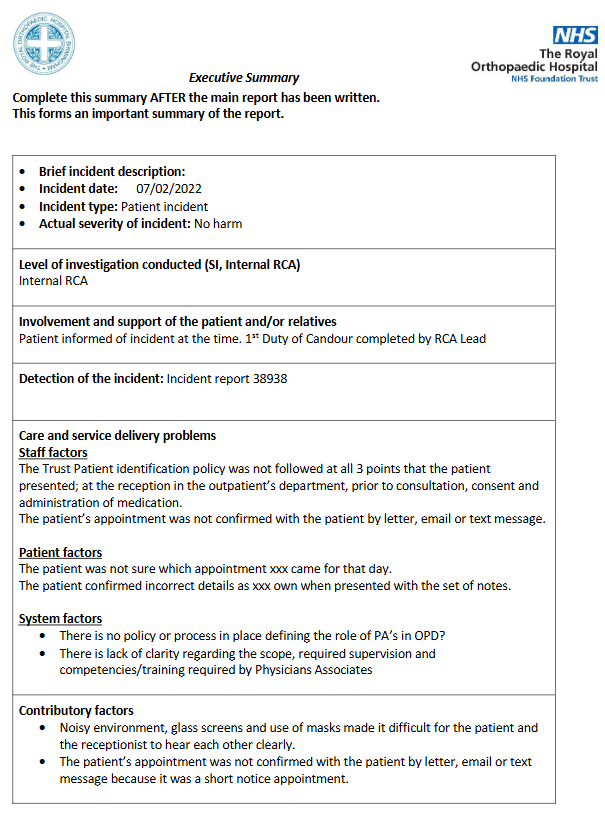
MAPs are not regulated. They have voluntary registers at a few Royal Colleges, but no statutory process to ensure they do not act dishonestly or recklessly to harm the public.
As a result, and an effectively unrestricted scope of practice, MAPs have been used in inappropriate roles—especially in the last few years. We have seen notable examples such as PAs involved in neurosurgery. Some of these say they are learning anatomy on the job.
It doesn't stop there. We have had deaths associated with PAs, following missed diagnoses like blood clots in the lung or torn blood vessels from the heart. In the case of Emily Chesterton, who died from a blood clot misdiagnosed as anxiety by a PA, the coroner ruled she likely..

...would have survived if she was referred to the hospital. Worse yet, her mother says that she didnt know she saw someone who wasn't a doctor. The title "physician associate" sounds grander than it's supervising General Practitioner.
The natural rebuttal to this is that "doctors make mistakes too". We know, and we try to prevent it at all costs. The difference is that we make mistakes with the gold standard of education and training. How does removing those standards for cheaper alternatives make sense?
Ah, but one further thing — they are not cheaper. A foundation doctor, who might oversee the work of a PA on a ward and prescribe for them, gets paid a salary of £28,274 pa for a 9-5 job. A first day PA would receive £35,392.
This is despite the fact there is usually no requirement for a PA to do night shifts, weekends or out of hours work. It is despite the fact they are less trained, cannot prescribe, cannot order radiation and cannot sign death certificates.
This situation is the equivalent, without any degree of irony, of a paralegal being paid more than a senior associate lawyer in many aspects. It is not far removed from a flight assistant out-earning the pilot, whilst having a go flying the plane.
Tomorrow morning, the statutory instrument process will see the regulation of PAs and AAs pass into law — failing a last minute U-turn from its Government majority. Some MPs are opposed, for example @KeeleyMP who was Emily's MP.
Statutory instruments are meant for technical pieces of legislation. They are almost always passed, in as little as 15-20 minutes. They were not intended for complex, controversial legislation like the regulation of potentially dangerous medical replacements.
Legal commentator David Allen Green has commented on them in depth, raising concerns about a lack of parliamentary scrutiny yet significant legal impact. They have been used for broad COVID regulations....
davidallengreen.com/2020/06/why-we…
davidallengreen.com/2020/06/why-we…
The question on everyone's lips in the medical profession is why these roles have been given such rapid prominence and power, despite lacking an evidence base proving their efficacy?
I say everyone's lips, but this is not exactly true. Multiple high level "leaders" of the medical profession have been involved in building this expert. Almost all of them refuse to acknowledge any concerns on safety — despite @TheDA_UK discovering over 680 concerns from doctors.
Concerns ranging from illegal prescribing, missed diagnoses including deaths, and replacing doctors on medical rotas. Why would institutions meant to protect the value of a doctor support these changes? That is a question that needs a deep dive, and some good journalism.
Tomorrow is all but a certainty — I hope that this introduction is raising some eyebrows amongst the public reading it. If you have butterflies saying "this can't be right" I assure you it is, and you, your family and friends are at risk of losing professional doctors.
I'll do my best to reply to questions tonight, as this is a brief introduction to far larger issues. I've hit the thread limit. I'm sure my colleagues will join in. Thank you, and please do raise these concerns with your MP - NOW - and please share this.
parliament.uk/get-involved/c…
parliament.uk/get-involved/c…
@carolvorders @CarolineLucas @LBC @BBCNews @BBCNewsnight @JanetEastham @BMA_JuniorDocs @MarinaPurkiss @Emmajourno @NickTriggle @AnaesUnited @iDrSunny @trishgreenhalgh @djnicholl @DrEilidhMaria @DrAsifQasim @mmamas1973 @BylineTimes @Dr_BellaR @Janmacd @Channel4News @doctor_oxford
@drcmday @mouseter_chef @Femi_Sorry @Xeon4f145d96s1 @DrAmirKhanGP @goldstone_tony @GoodLawProject @JolyonMaugham @RosieisaHolt @HelenRSalisbury @davidhencke @VirtueOfNothing @keepnhspublic @parthaskar @DrLindaDykes @DrLKVaughan @ShaunLintern @GMB @mancunianmedic @maitlis
@GBNEWS @itvnews @SkyNews @PaulaMc007 @teekayoki @ObaBabsOsibodu @drphiliplee1 @PeterStefanovi2 @quackophage @r1chardf1tzg3r1 @RoshanaMN @dr_shibley @dgraemestewart @drokane @DrSteveTaylor @PPJSucharitkul @lizzie_toberty @TheDA_UK @theJeremyVine @WB_UK @drmeenalviz @veggieequallife @VikiLovesFACS @_VivekTrivedi @RobLaurensonD4P @DrDavidRouse @wanderingwelch @jfdwolff @guardian @doctor_katie @katlay @michaelsearles_ @LBCNews @BBCNewsPR @SkyNewsBreak @MarikaSboros @mjauk @HSJnews @FinancialTimes
@guardian decided to post an incredibly one sided story of PAs at Royal Berkshire NHS Trust. It didn't seek comment from an organisation that has collected concerns on PAs for months. I have responded below:
https://twitter.com/drmattuk/status/1747892128955478168?t=KgFHSO7aAYhx4fD843xIYw&s=19
• • •
Missing some Tweet in this thread? You can try to
force a refresh