
A ( long but I think worth reading) thread on Gynecologic Surgical reimbursement and how it affects all of us:
Gynecologic surgeons are the lowest paid surgeons in medicine, and the gap between us and other surgeons is widening. This disincentivizes the recruitment of clinical and research talent into our high-demand field, but in a profit-driven medical environment--

--disincentivizes health care systems from providing Gyn surgical care, and providing Gyn surgeons with OR time, facilities, and staff. This leads to patient harm due to high wait times for surgery, inconsistent surgical teams, decreased surgery volume, and worse outcomes.
General OB/Gyns train for 4 years, and most are low volume surgeons, doing 1-5 hysterectomies per year. This leads to higher complication rates. Sub-specialist Gyn Surgeons (Gyn Onc, Urogyn, MIGS) complete 2-4 years of additional surgical training in advanced Gyn surgery.
We often as a result have more surgical training than our higher paid surgeon colleagues (orthopedics, urology, etc). We have exceptionally low complication rates, but our reimbursement is far lower than the market standard of other surgical disciplines.
As a result, the resources we can provide for our patients is fewer. How did we get here? The Social Security Act in the 1990s restablished the relative value unit (RVU) system. Under the SSA, US Health and Human Services asked the Harvard School of Public Health to conduct--
A study to establish initial comparable set points for how much common procedures would be reimbursed. Gyn surgery was barely addressed in these original set point and undervalued from the start.
The RVU system was originally created for medicare and medicaid, but now it provides the framework for all insurer reimbursement. Not only are Gyn surgical procedures reimbursed profoundly low, but often the number of DOLLARS PER RVU is lower for someone with Gyn training.
This means that as a Urogynecologist, the same sling surgery that I do that a Urologist does for the exact same number of RVUs will generate less money.
RVUs for each procedure are decided by the AMA RVU committee (RUC) and the Centers for Medicaid and Medicare services (CMS) @CMSGov accepts approximately 80% of the RUCs recommendations. BUT what is important to note about the RUC are three things:
1) There is a budget neutrality clause that says that there is a FINITE number of RVUS in medicine, so to have one procedure go up in value, another has to come down
2) OB/Gyn has only one vote, appointed by ACOG, an organization that favors general OB/Gyns and OB services
2) OB/Gyn has only one vote, appointed by ACOG, an organization that favors general OB/Gyns and OB services
3) There are only 5 women on the 32 member RUC committee!
So, to value Gyn surgery more, RVUS need to be taken away either from OB (which is also undervalued) or another specialty, which rarely happens.
So, to value Gyn surgery more, RVUS need to be taken away either from OB (which is also undervalued) or another specialty, which rarely happens.
Multiple reports have shown that equivalent procedures done on women vs. men (like in Gynecology vs. Urology), that male procedures reimburse on average 30% more. So the discrimination is baked into the coding; women's bodies are, according to the RVU system, worth less than men.
The other way in which this profoundly impacts Gyn Surgeons is the fact that female surgeons already make 70% of what male surgeons do. Since the majority of Gyn surgeons are women, this is a double-whammy of pay discrimination.
Briefly, some examples: an endometriosis excision, which can take 1-8 hours of complex surgical time by an expert MIGS surgeon, bills 12.15 RVUs. A shoulder arthroscopy, which takes 30 minutes-1 hour, bills 15 RVUs. You can see how hospitals would quickly prioritize orthopedics.
So what are some solutions? The easiest thing to do would be for @HHSGov and @XavierBecerra to produce a report that shows that budget neutrality is hurting women and change the policy around a zero sum game for medical reimbursement.
Gyn surgical groups like @GynSurgery also will be imperative to create a study similar to the Harvard SPH study from the early 1990s re-evaluating appropriate reimbursement for Gyn surgery.
This point is, this has to change, and fast. My colleagues across the country are facing daily challenges for hundreds of their patients who can't get surgery because the Gyn Surgeons aren't given surgical time in operating rooms because their surgeries "aren't worth it".
Endometriosis patients are waiting years for surgery, prolapse case time waits are 3-6 months, Gyn Oncologists also struggle for time. The alternative is that Gyn Surgeons take cash instead of insurance, leaving women who can't pay in the complete dark.
We have to decide within medicine and society that women's bodies have value--AND THEY DO. Women keep the rest of us healthy, but while they live longer, they live in worse health than men for the last decades of their life.
A lot of this disparity is due to devaluation of women's healthcare inside of the systems that provide it. The last thing I want to say is that this is a large reason that women's health research has lagged behind.
Due to the immense amount of clinical work OB/Gyn's have to do to maintain their employment (a SMALL field, training maybe 10 residents per program per year, almost half of whom do a fellowship while the rest are expected to do the lion's share of women's heath provision--
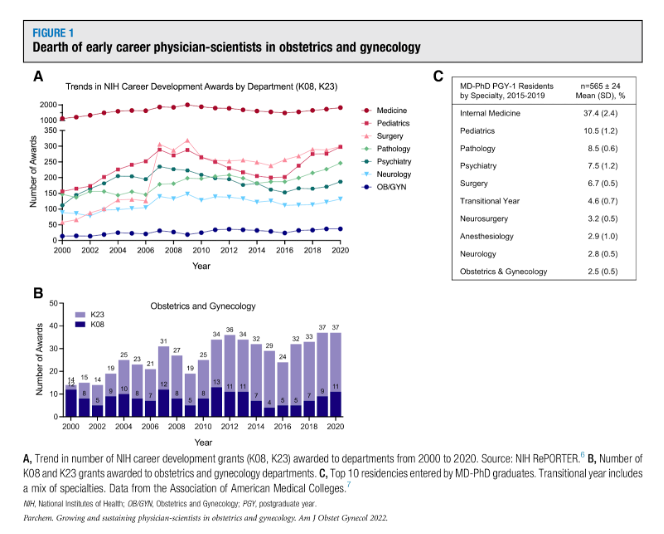
It leaves a dearth of time for research. Ob/Gyn has the lowest number of Career Development Awards of any medical field, as below. As a society, we NEED to support women and their doctors before it is too late. 
@nytimes @NYTScience @BuzzFeed @washingtonpost @HuffPostWomen @HuffPost @FLOTUS @MichelleObama @NBCNewsHealth
• • •
Missing some Tweet in this thread? You can try to
force a refresh




