UCSF’s Jack Turban (@jack_turban) and Yale’s Meredithe McNamara recently criticized a new Finnish study that further weakens the “suicide prevention” narrative.
Their criticisms are wrong and hypocritical.
Here’s why. 🧵
Their criticisms are wrong and hypocritical.
Here’s why. 🧵
To recall, the Finnish study found that suicide in gender clinic-referred (GR) youths <23 was uncommon (0.3%), and when the model adjusted for severe psychiatric comorbidities, there was no statistically significant difference in suicide rates between GR youth and controls. /2
The study's implication is that suicide prevention should focus on comorbid psychiatric problems that frequently occur in dysphoric youth, not on modifying the body’s sex characteristics. /3
See the study here:
SEGM’s analysis:
mentalhealth.bmj.com/content/27/1/e…
segm.org/Suicide-Gender…
See the study here:
SEGM’s analysis:
mentalhealth.bmj.com/content/27/1/e…
segm.org/Suicide-Gender…
Turban said the Finns are “very stupid or intentionally misleading" because they controlled for psychiatric problems. His unstated assumption is that psychiatric problems are simply the result of “unaffirmed” gender identity—also known as the “minority stress” hypothesis. /4 
Turban's use of "minority stress" is untested, clinically dangerous (as we've seen from whistleblowers and other sources), and self-serving. I’m happy to debate it with him if he so wishes. /5
Littman, Biggs and I touch on the issue briefly here:
link.springer.com/article/10.100…
Littman, Biggs and I touch on the issue briefly here:
link.springer.com/article/10.100…
Turban’s adherence to "minority stress" is so dogmatic that he once claimed that it causes autism-like symptoms, which explains the overrepresentation of such symptoms in gender dysphoric/trans-identified youth. In effect, Turban claimed that by transitioning kids you can eliminate autism-like traits. /6
linkinghub.elsevier.com/retrieve/pii/S…
linkinghub.elsevier.com/retrieve/pii/S…
Turban’s argument drew criticism from fellow gender clinicians, transgender researchers and transgender advocates—including the Dutch pioneers of pediatric gender medicine themselves. Turban’s argument that what looks like autism is really untreated gender dysphoria, they said, is “counterproductive and not contributing to better care for those who need it.” /7
jaacap.org/article/S0890-…
jaacap.org/article/S0890-…
A group of 21 trans-advocate researchers also wrote to the journal (@JAACAP) about Turban’s paper, stating, “We are concerned that perpetuating misunderstanding about the co-occurrence [of autistic traits and gender dysphoria] places individuals at risk.” /8
experts.umn.edu/en/publication…
experts.umn.edu/en/publication…
To state the obvious, any stat analysis that fails to control for confounders is flawed. Severe mental illness is a key predictor of suicide. If one does not control for it, how can one distinguish possible drivers of suicide (e.g., gender distress vs bipolar disorder)? /9
Meredithe McNamara, who chimed in through trans activist Erin Reed’s blog, claimed that controlling for psychiatric problems in gender medicine is like controlling for hours worked in the analysis of pay gender gap. It’s possible, McNamara says, that women work fewer hours (and thus on average make less than men) because of "gendered expectations" around how much to work. /10

McNamara’s logic is flawed. If there is a disparity between men and women in terms of average work hours, this obviously must be accounted for when comparing pay. That doesn't mean it has to be the final word. If McNamara is right about "gendered expectations" (whatever she means by that) shaping work hours, fine, define that murky term, test it empirically, and be open to the possibility that women work fewer hours for reasons other than sexism. But to suggest that researchers shouldn't control for hours worked is silly and unscientific. It's reasoning backwards from your preferred conclusion ("gendered expectations"). /11
Back to the Finnish study. Could the Finnish statistical model be further improved? If Jack has a suggestion, he should write a letter to the editor and suggest his critique. In calling his international colleagues “stupid” and “misleading,” Jack may be giving a masterclass in projection. Let’s examine his own research. /12
In his study on puberty blockers’ effect on suicidality, Turban used the exact method he is accusing the Finnish researchers of using. If a variable was associated with suicidality, he controlled for it in the model. This included family support, employment, income, relationships, and even gender identity. /13
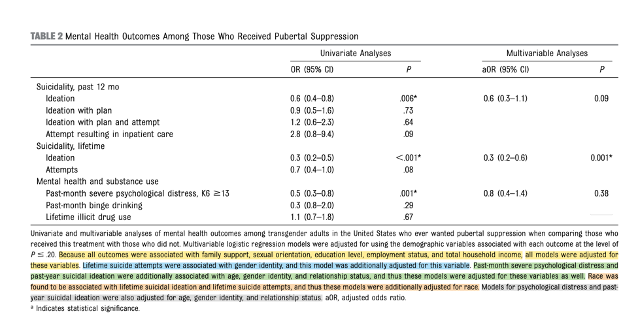
The 2020 study was subject to multiple criticisms. One was that Turban did not control for mental illness, measured in the study by the “severe psychological distress” variable (score of 13+ on the K6 scale). Why did Turban control for other variables associated with suicidality but not this one? Perhaps he feared that the "live-saving” properties of puberty blockers might disappear if severe mental illnesses was controlled for. /14
Could the Finnish model have been further improved upon? Likely, yes. If Turban has better ideas, he can suggest them through respectful, scholarly debate, just as dozens of researchers (myself included) have written letters to the editor to discuss the flaws in his research. That’s how science works. /15
The dishonesty and incompetence of prominent gender clinicians like Turban and McNamara never ceases to amaze me. I expect this from activists who pass themselves off as journalists and who consistently spread misinformation, but Turban and McNamara are physicians who treat children and have the power to shape medical policy. /16
You’d think that activists like Turban would be extremely pleased at learning that suicide (which is different from “suicidality”) is actually very uncommon among trans-identified young people, even if it is elevated relative to the general population. Instead, their response to the Finnish study and others like it (e.g., Biggs 2022) has been disappointment, even outrage. /17
That tells you something about why they use the suicide narrative. It’s not because they actually believe trans-identified teens are at high risk for suicide and want to prevent it. It’s because the threat of suicide is useful: for bullying parents into agreeing to risky and experimental medical interventions for their kids, for pressuring policymakers to allow gender clinicians regulate themselves, and for getting allied journalists to feel that they too are life-saving heroes. /end
• • •
Missing some Tweet in this thread? You can try to
force a refresh